Gastroenterology Department, Great Ormond Street Hospital, London, UK.
Paediatric Department, "V. Buzzi" Children's Hospital, University of Milan, Milan, Italy.
Clin Transl Gastroenterol. 2023 Mar 1;14(3):e00544. doi: 10.14309/ctg.0000000000000544.
Split-dose thiopurine and allopurinol-thiopurine cotherapy strategies have been suggested as rescue therapeutic options for children with inflammatory bowel disease (IBD) and impaired thiopurine metabolism. We compared the efficacy and safety of these regimens in patients who previously failed conventional thiopurine treatment.
Children with IBD treated with split-dose thiopurine or low-dose thiopurine-allopurinol cotherapy were retrospectively identified. Medical records were reviewed for demographics, treatment regimen, reason for thiopurine failure, side effects, and discontinuation of treatment. Laboratory findings were evaluated at different time points.
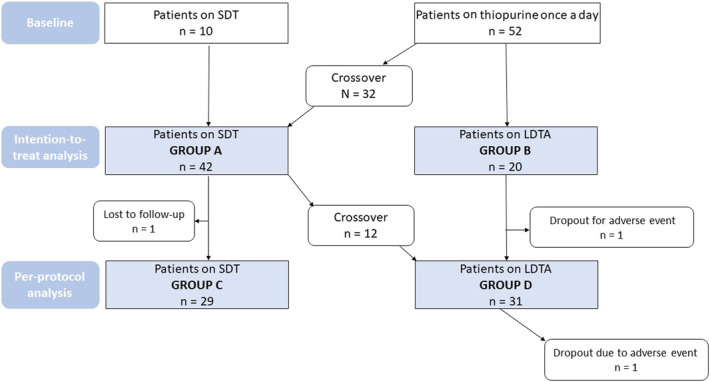
After prior therapeutic failure, 42 patients were on split-dose regimen (group A) and 20 patients were on thiopurine-allopurinol cotherapy (group B). Twelve patients crossed from group A to group B because of treatment failure, 1 patient was lost at follow-up, and 1 patient discontinued the treatment. The final cotherapy group comprised 29 children (group C), while the split-dose group (group D) included 31 children. Intention-to-treat analysis showed significant differences between split-dose regimen and thiopurine-allopurinol cotherapy for 6-thioguanine nucleotide (6-TGN)/6-methyl mercaptopurine (6-MeMP) ratio ( P < 0.001), 6-TGN ( P < 0.05), and 6-MeMP ( P < 0.001) at 1-3 months. As per protocol analysis, there was a significant difference between group C and group D at 6 months for 6-MeMP ( P < 0.05) and 6-TGN/6-MeMP ratio ( P < 0.05) and at 12 months for 6-MeMP ( P < 0.05) and 6-TGN/6-MeMP ratio ( P < 0.001). Side effects were more frequent in allopurinol-thiopurine cotherapy ( P < 0.05).
In children with IBD and impaired thiopurine metabolism, split-dose thiopurine and low-dose thiopurine-allopurinol cotherapy are both effective therapeutic strategies. The latter shows higher efficacy but a higher side effect rate, suggesting the use of split-dose regimen as the first-line approach.
对于存在巯嘌呤代谢异常的炎症性肠病(IBD)患儿,已提出采用分次给予巯嘌呤和别嘌醇-巯嘌呤联合治疗作为补救性治疗选择。我们比较了这些方案在先前常规巯嘌呤治疗失败的患者中的疗效和安全性。
回顾性确定接受分次给予巯嘌呤或低剂量巯嘌呤-别嘌醇联合治疗的 IBD 患儿。评估了人口统计学、治疗方案、巯嘌呤治疗失败的原因、副作用和治疗中断情况。在不同时间点评估了实验室检查结果。
在先前的治疗失败后,42 名患者接受了分次剂量方案(A 组),20 名患者接受了巯嘌呤-别嘌醇联合治疗(B 组)。由于治疗失败,12 名患者从 A 组转为 B 组,1 名患者失访,1 名患者停止治疗。最终联合治疗组包括 29 名儿童(C 组),而接受分次剂量方案的组(D 组)包括 31 名儿童。意向治疗分析显示,在 6-巯基嘌呤核苷酸(6-TGN)/6-甲基巯基嘌呤(6-MeMP)比值(P<0.001)、6-TGN(P<0.05)和 6-MeMP(P<0.001)方面,分次剂量方案与巯嘌呤-别嘌醇联合治疗在 1-3 个月时存在显著差异。根据方案分析,在 6 个月时,C 组与 D 组在 6-MeMP(P<0.05)和 6-TGN/6-MeMP 比值(P<0.05)方面存在显著差异,在 12 个月时在 6-MeMP(P<0.05)和 6-TGN/6-MeMP 比值(P<0.001)方面存在显著差异。别嘌醇-巯嘌呤联合治疗的副作用更为频繁(P<0.05)。
在存在巯嘌呤代谢异常的 IBD 患儿中,分次给予巯嘌呤和低剂量巯嘌呤-别嘌醇联合治疗均为有效的治疗策略。后者显示出更高的疗效,但副作用发生率更高,这提示采用分次剂量方案作为一线治疗方法。