Global Health Fellow UCGHI, San Francisco, CA, USA.
Kenyatta University School of Medicine, P.O.BOX 43844 00100, Nairobi, Kenya.
BMC Pregnancy Childbirth. 2017 Nov 17;17(1):387. doi: 10.1186/s12884-017-1566-3.
Despite recent advances in surgery and anaesthesia which significantly improve safety, many health facilities in low-and middle-income countries (LMICs) remain chronically under-resourced with inability to cope effectively with serious obstetric complications (Knight et al., PLoS One 8:e63846, 2013). As a result many of these countries still have unacceptably high maternal and neonatal mortality rates. Recent data at the national referral hospitals in East Africa reported that none of the national referral hospitals met the World Federation of Societies of Anesthesiologists (WFSA) international standards required to provide safe obstetric anaesthesia (Epiu I: Challenges of Anesthesia in Low-and Middle-Income Countries. WFSA; 2014 http://wfsa.newsweaver.com/Newsletter/p8c8ta4ri7a1wsacct9y3u?a=2&p=47730565&t=27996496 ). In spite of this evidence, factors contributing to maternal mortality related to anaesthesia in LMICs and the magnitude of these issues have not been comprehensively studied. We therefore set out to assess regional referral, district, private for profit and private not-for profit hospitals in Uganda.
We conducted a cross-sectional survey at 64 government and private hospitals in Uganda using pre-set questionnaires to the anaesthetists and hospital directors. Access to the minimum requirements for safe obstetric anaesthesia according to WFSA guidelines were also checked using a checklist for operating and recovery rooms.
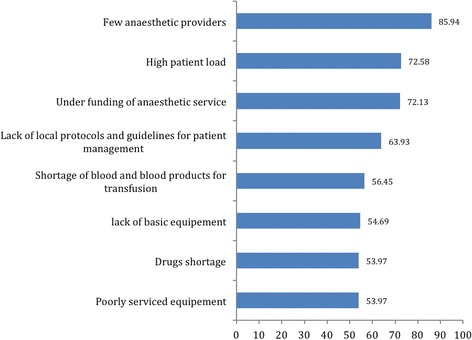
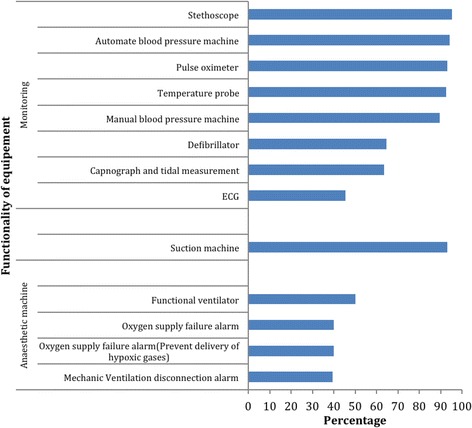
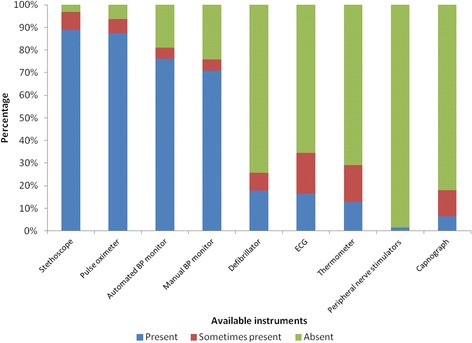
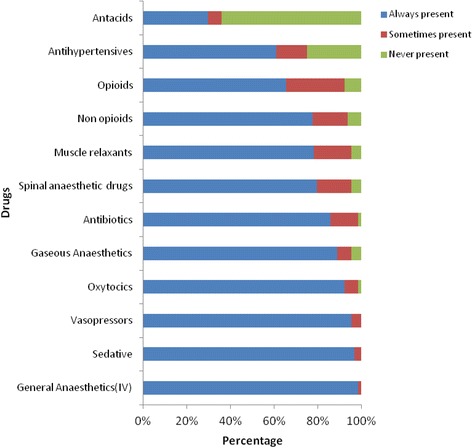
Response rate was 100% following personal interviews of anaesthetists, and hospital directors. Only 3 of the 64 (5%) of the hospitals had all requirements available to meet the WFSA International guidelines for safe anaesthesia. Additionally, 54/64 (84%) did not have a trained physician anaesthetist and 5/64 (8%) had no trained providers for anaesthesia at all. Frequent shortages of drugs were reported for regional/neuroaxial anaesthesia, and other essential drugs were often lacking such as antacids and antihypertensives. We noted that many of the anaesthesia machines present were obsolete models without functional safety alarms and/or mechanical ventilators. Continuous ECG was only available in 3/64 (5%) of hospitals.
We conclude that there is a significant lack of essential equipment for the delivery of safe anaesthesia across this region. This is compounded by the shortage of trained providers and inadequate supervision. It is therefore essential to strengthen anaesthesia services by addressing these specific deficiencies. This will include improved training of associate clinicians, training more physician anaesthetists and providing the basic equipment required to provide safe and effective care. These services are key components of comprehensive emergency obstetric care and anaesthetists are crucial in managing critically ill mothers and ensuring good surgical outcomes.
尽管最近在手术和麻醉方面取得了重大进展,显著提高了安全性,但许多中低收入国家(LMICs)的医疗设施仍然长期资源不足,无法有效应对严重的产科并发症(Knight 等人,PLoS One 8:e63846,2013 年)。结果,这些国家中有许多国家的母婴死亡率仍然高得不可接受。东非国家转诊医院的最新数据报告称,没有一家国家转诊医院符合世界麻醉师协会联合会(WFSA)提供安全产科麻醉所需的国际标准(Epiu I:麻醉在中低收入国家面临的挑战。WFSA;2014 年 http://wfsa.newsweaver.com/Newsletter/p8c8ta4ri7a1wsacct9y3u?a=2&p=47730565&t=27996496)。尽管有这方面的证据,但导致 LMICs 中与麻醉相关的孕产妇死亡的因素以及这些问题的严重程度尚未得到全面研究。因此,我们着手评估乌干达的区域转诊、地区、私立营利性和私立非营利性医院。
我们对乌干达的 64 家政府和私立医院进行了横断面调查,使用预先设定的问卷对麻醉师和医院院长进行了调查。还使用 WFSA 指南的操作和恢复室检查表检查了获得安全产科麻醉最低要求的情况。
对麻醉师和医院院长进行了个人访谈后,回复率为 100%。64 家医院中只有 3 家(5%)具备满足 WFSA 国际安全麻醉指南的所有要求。此外,54/64(84%)没有经过培训的医师麻醉师,5/64(8%)根本没有经过培训的麻醉师。据报道,区域/神经轴麻醉经常出现药物短缺,其他基本药物经常缺乏,如抗酸剂和降压药。我们注意到,许多现有的麻醉机都是没有功能安全警报和/或机械呼吸机的过时型号。只有 3/64(5%)的医院提供连续心电图。
我们的结论是,该地区在提供安全麻醉方面存在严重缺乏基本设备的问题。这因训练有素的提供者短缺和监督不足而更加复杂。因此,必须通过解决这些具体缺陷来加强麻醉服务。这将包括改善助理临床医生的培训、培训更多的医师麻醉师以及提供提供安全有效的护理所需的基本设备。这些服务是综合紧急产科护理的关键组成部分,麻醉师在治疗重症产妇和确保良好手术结果方面发挥着至关重要的作用。