Centre for Radiation Oncology KSA-KSB, Kantonsspital Aarau AG, Tellstrasse, CH-5001, Aarau, Switzerland.
Centre for Hematology and Oncology, University Hospital Zurich, Zürich, Switzerland.
Radiat Oncol. 2017 Nov 21;12(1):183. doi: 10.1186/s13014-017-0923-8.
Pancreatic cancer has a dismal prognosis with 5-year overall survival rate of around 5%. Although surgery is still the best option in operable cases, majority of the patients who present in locally advanced stages are deemed inoperable. Novel approaches are therefore needed for the management of around 80% of these inoperable locally advanced pancreatic cancers (LAPC). Hyperthermia (39-43 °C) is a potent radiosensitizer and further enhances the action of gemcitabine, also a known radiosensitizer. Thus through triple sensitization, a combination of hyperthermia, radiotherapy and gemcitabine could be expected to improve the therapeutic outcomes in LAPC.
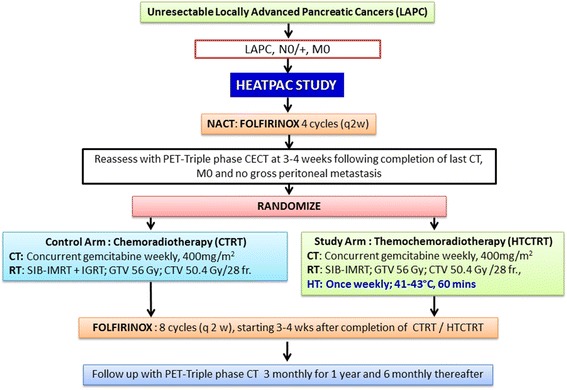
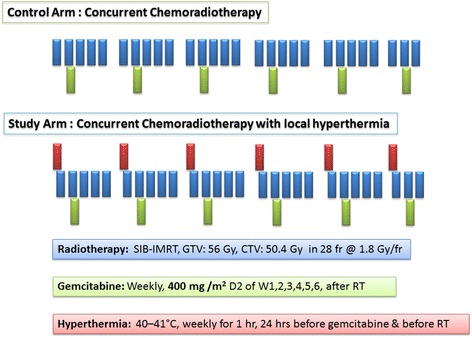
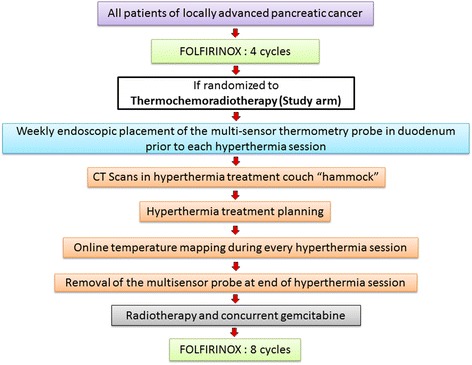
This phase II randomized trial, HEATPAC in unresectable LAPC, explores the feasibility and efficacy of concurrent thermochemoradiotherapy (HTCTRT) over chemoradiotherapy (CTRT) alone with pre- and post-intervention FOLFIRINOX at standard dosage and schedule. Following 4 cycles of neoadjuvant FOLFIRINOX, patients with no metastasis and absence of gross peritoneal carcinomatosis would be randomized to either (a) control arm: concurrent CTRT with gemcitabine (400 mg/m, weekly ×6) or (b) study arm: locoregional hyperthermia (weekly ×6 during radiotherapy) with concurrent CTRT (same as in control arm). All patients would receive simultaneous-integrated boost intensity-modulated radiation therapy to doses of 56Gy and 50.4Gy to the gross and clinical target volumes respectively delivered in 28 fractions over 5.5 weeks. Deep locoregional hyperthermia would be administered weekly and monitored with real-time intraduodenal multisensor thermometry probe. A temperature of 40-43 °C for 60 min would be aimed for each hyperthermia session. On completion of CTRT/HTCTRT, patients of both groups would receive an additional 8 cycles of FOLFIRINOX.
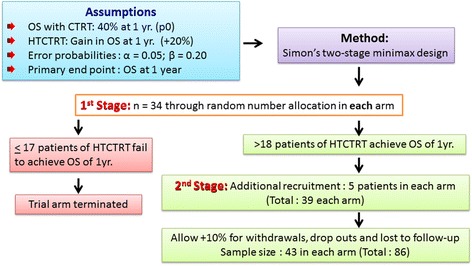
The expected 1-year baseline overall survival with CTRT alone is considered as 40%. With HTCTRT, a survival advantage of +20% is expected. Considering α = 0.05 and β = 0.80 for sample size computation, a total of 86 patients would be equally randomized into the two treatment groups. This phase II study if found to be safe and effective, would form the basis of a future phase III randomized study.
The trial has been registered with the ClinicalTrials.gov ( NCT02439593 ). The study has been approved by the Ethical Commissions of Basel and Zurich and is open for patient recruitment.
胰腺癌预后极差,5 年总生存率约为 5%。尽管手术仍是可手术病例的最佳选择,但大多数局部晚期病例仍被认为无法手术。因此,需要新的方法来治疗大约 80%的这些无法手术的局部晚期胰腺癌(LAPC)。热疗(39-43°C)是一种有效的放射增敏剂,进一步增强了吉西他滨的作用,吉西他滨也是一种已知的放射增敏剂。因此,通过三重增敏作用,热疗、放疗和吉西他滨的联合应用有望改善 LAPC 的治疗效果。
本项 II 期随机试验 HEATPAC 研究了不可切除的 LAPC 中同步热化疗(HTCTRT)与单纯化疗(CTRT)联合新辅助 FOLFIRINOX 方案(标准剂量和方案)的可行性和疗效。在 4 个周期的新辅助 FOLFIRINOX 治疗后,无转移和无明显腹膜癌病的患者将被随机分配到以下两组之一:(a)对照组:同步 CTRT 联合吉西他滨(400mg/m,每周 6 次);(b)研究组:局部热疗(每周 6 次,放疗期间)联合同步 CTRT(与对照组相同)。所有患者均接受同时调强放疗,总剂量为 56Gy 和 50.4Gy,分别给予 28 次,每次 5.5 周。深部局部热疗每周进行一次,并通过实时十二指肠内多传感器温度探头进行监测。每次热疗的目标温度为 40-43°C,持续 60 分钟。完成 CTRT/HTCTRT 后,两组患者均接受额外 8 个周期的 FOLFIRINOX 治疗。
单独接受 CTRT 的患者预计 1 年的基线总生存率为 40%。如果接受 HTCTRT,预计生存优势将增加 20%。考虑到样本量计算的 α=0.05 和 β=0.80,共需要 86 例患者等分为两组。如果这项 II 期研究被证明是安全有效的,它将为未来的 III 期随机研究奠定基础。
该试验已在 ClinicalTrials.gov(NCT02439593)注册。该研究已获得巴塞尔和苏黎世伦理委员会的批准,并正在招募患者。