Theron Annette J, Anderson Ronald, Rossouw Theresa M, Steel Helen C
Faculty of Health Sciences, Department of Immunology, Institute for Cellular and Molecular Medicine, University of Pretoria, Pretoria, South Africa.
Tshwane Academic Division of the National Health Laboratory Service, Pretoria, South Africa.
Front Immunol. 2017 Nov 2;8:1461. doi: 10.3389/fimmu.2017.01461. eCollection 2017.
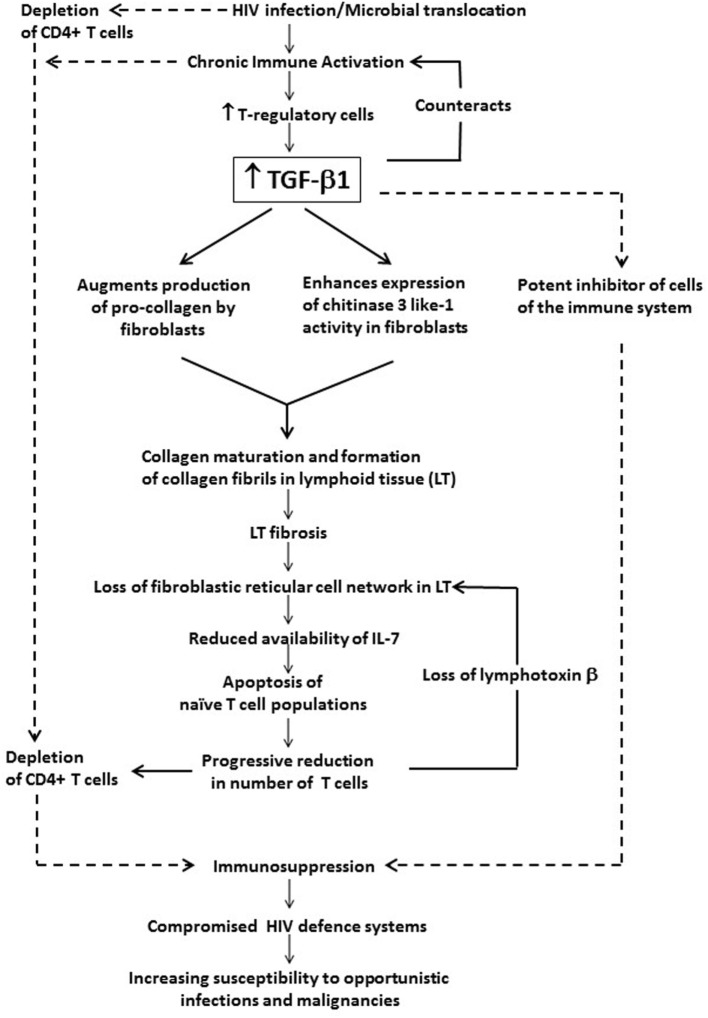
Even after attainment of sustained viral suppression following implementation of highly active antiretroviral therapy, HIV-infected persons continue to experience persistent, low-grade, systemic inflammation. Among other mechanisms, this appears to result from ongoing microbial translocation from a damaged gastrointestinal tract. This HIV-related chronic inflammatory response is paralleled by counteracting, but only partially effective, biological anti-inflammatory processes. Paradoxically, however, this anti-inflammatory response not only exacerbates immunosuppression but also predisposes for development of non-AIDS-related, non-communicable disorders. With respect to the pathogenesis of both sustained immunosuppression and the increased frequency of non-AIDS-related disorders, the anti-inflammatory/profibrotic cytokine, transforming growth factor-β1 (TGF-β1), which remains persistently elevated in both untreated and virally suppressed HIV-infected persons, may provide a common link. In this context, the current review is focused on two different, albeit related, harmful activities of TGF-β1 in HIV infection. First, on the spectrum of anti-inflammatory/immunosuppressive activities of TGF-β1 and the involvement of this cytokine, derived predominantly from T regulatory cells, in driving disease progression in HIV-infected persons both non-fibrotic and profibrotic mechanisms. Second, the possible involvement of sustained elevations in circulating and tissue TGF-β1 in the pathogenesis of non-AIDS-defining cardiovascular, hepatic, pulmonary and renal disorders, together with a brief comment on potential TGF-β1-targeted therapeutic strategies.
即使在实施高效抗逆转录病毒疗法后实现了持续的病毒抑制,HIV感染者仍持续经历持续性、低度全身性炎症。在其他机制中,这似乎是由于受损胃肠道持续发生微生物易位所致。这种与HIV相关的慢性炎症反应伴随着起抵消作用但仅部分有效的生物抗炎过程。然而,矛盾的是,这种抗炎反应不仅会加剧免疫抑制,还会增加非艾滋病相关非传染性疾病的发病风险。关于持续免疫抑制和非艾滋病相关疾病发病率增加的发病机制,抗炎/促纤维化细胞因子转化生长因子-β1(TGF-β1)在未治疗和病毒抑制的HIV感染者中均持续升高,可能提供了一个共同的联系。在此背景下,本综述聚焦于TGF-β1在HIV感染中的两种不同但相关的有害作用。首先,是TGF-β1的抗炎/免疫抑制活性谱以及这种主要来源于调节性T细胞的细胞因子在驱动HIV感染者疾病进展中的作用——包括非纤维化和促纤维化机制。其次,循环和组织中TGF-β1持续升高可能参与非艾滋病定义的心血管、肝脏、肺部和肾脏疾病的发病机制,并简要评论针对TGF-β1的潜在治疗策略。