Novartis Pharma AG, Basel, Switzerland.
QuintilesIMS, Frankfurt, Germany.
Adv Ther. 2017 Dec;34(12):2585-2600. doi: 10.1007/s12325-017-0624-6. Epub 2017 Nov 21.
Anti-vascular endothelial growth factor therapy is the standard of care for neovascular age-related macular degeneration (nAMD). The dosage of two licensed agents, ranibizumab and aflibercept, was established through clinical trials; however, it is unclear if either agent is administered as recommended in routine clinical practice. Using pharmacy claims data, we investigated if the dispensing patterns of ranibizumab differ from those of aflibercept 6 and 12 months after treatment initiation.
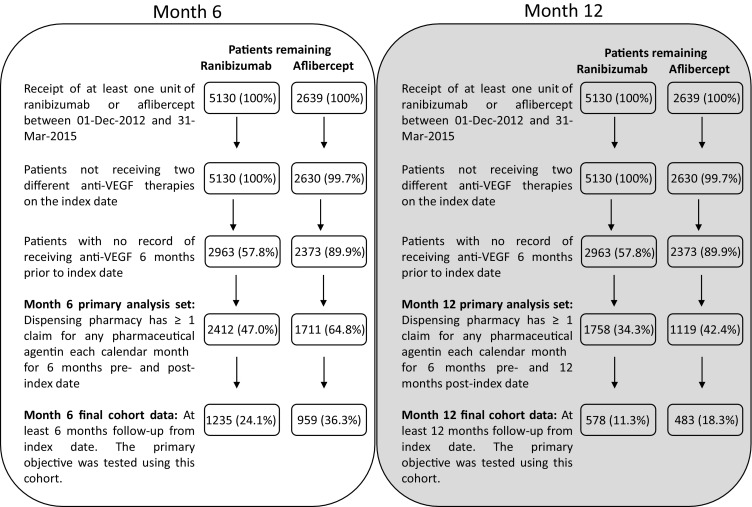
Prescription data retrieved from the Australian IMS AUS LRx database were used to identify nAMD patients with one or more claims for ranibizumab or aflibercept between December 1, 2012, and March 31, 2015, with follow-up of at least 6 months. The number of ranibizumab and aflibercept units dispensed was adjusted for baseline patient Medication-Based Disease Burden Index (MBDBI) scores. No difference in the number of ranibizumab versus aflibercept units dispensed was concluded if the 95% confidence interval (CI) limits of the adjusted mean difference between the study cohorts were 1.00 unit or less.
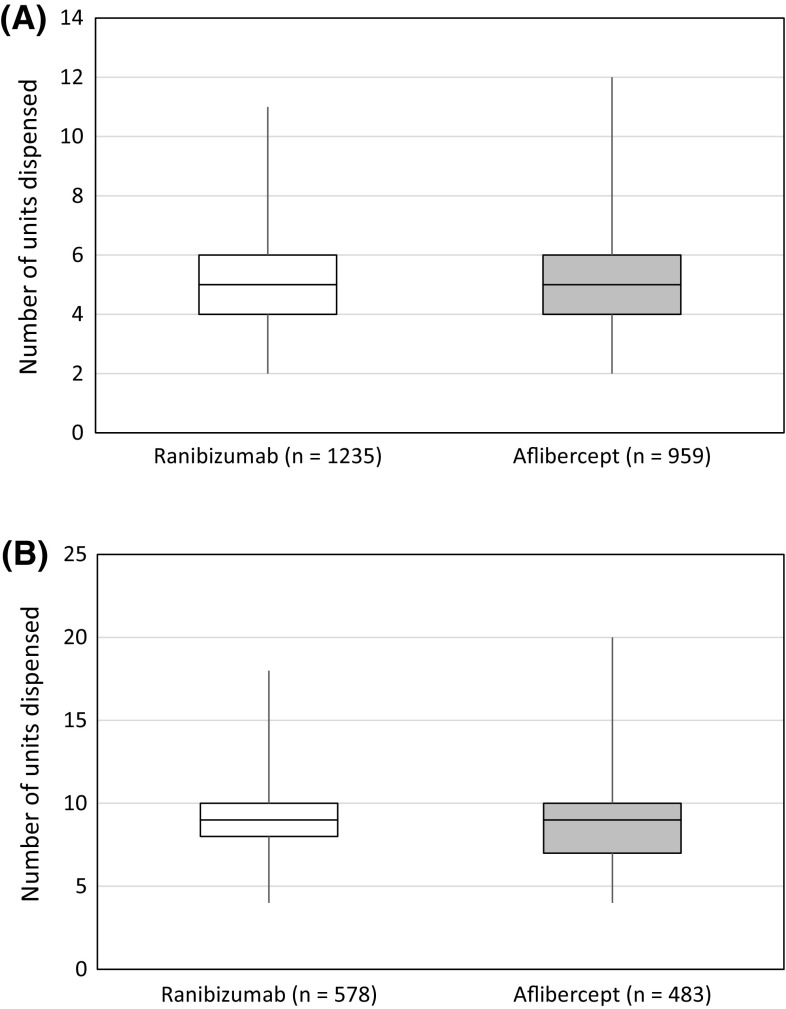
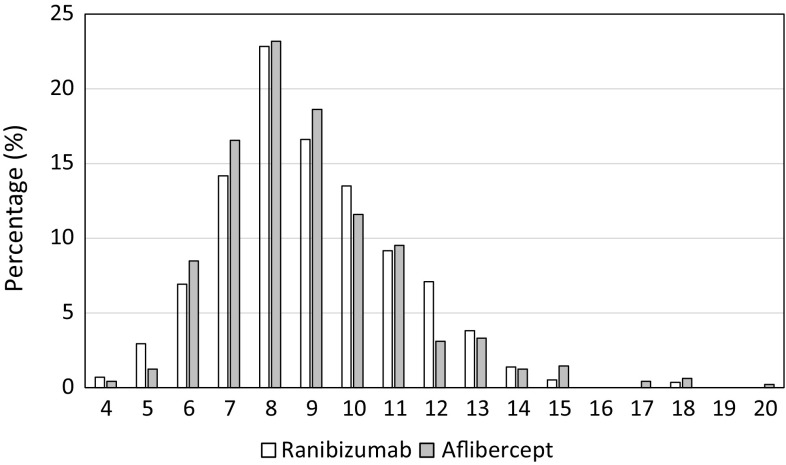
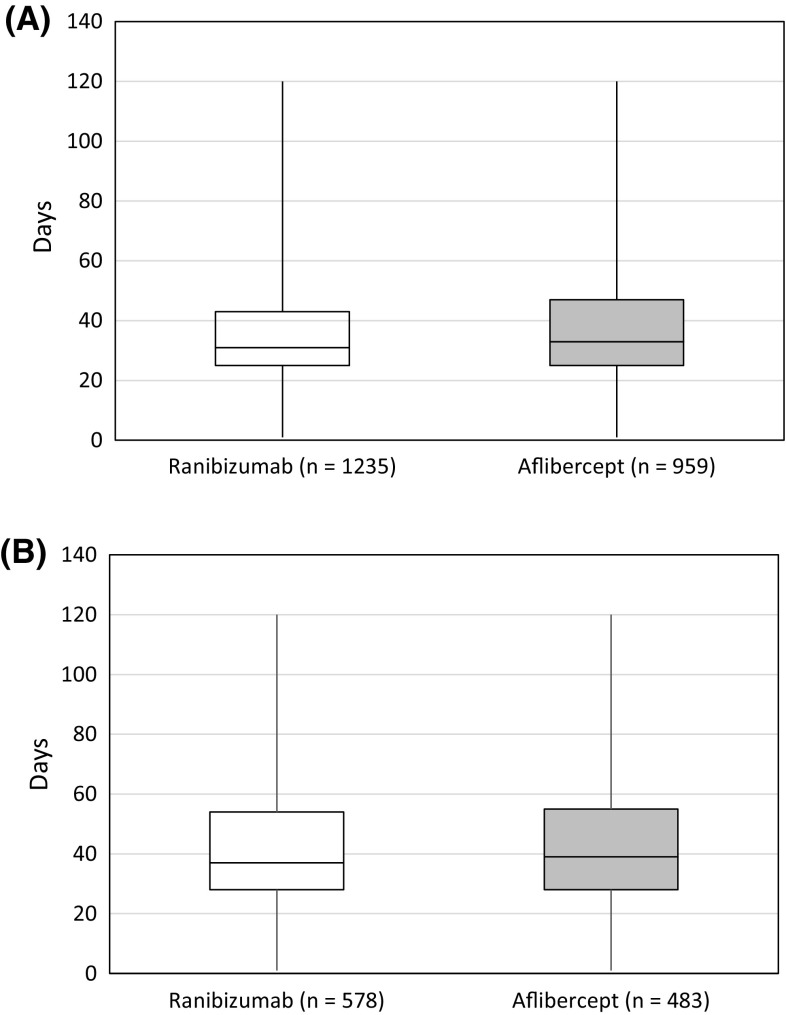
Baseline patient MBDBI scores were similar for the ranibizumab (N = 1235) and aflibercept (N = 959) cohorts. The adjusted mean (standard deviation) number of units dispensed was 5.3 (1.3) versus 5.1 (1.4) at month 6 and 8.9 (2.2) versus 8.9 (2.3) at month 12. The 95% CI limits of the adjusted mean difference did not exceed 1.00 unit dispensed at either time point: 95% CI of 0.09 to 0.32 for an adjusted mean difference of 0.20 at month 6 and -0.23 to 0.30 for an adjusted mean difference of 0.04 at month 12. Mean (standard deviation) dispensing intervals were comparable for both cohorts: 35.3 (19.2) days versus 36.8 (20.0) days at month 6 (adjusted mean difference -1.59 days; 95% CI -2.51 to -0.67 days) and 41.2 (20.9) days versus 41.6 (20.4) days at month 12 (adjusted mean difference -0.40 days; 95% CI -1.70 to 0.91 days).
Ranibizumab and aflibercept are dispensed in a similar manner by Australian pharmacies during the first year of treatment.
Novartis Pharma AG.
抗血管内皮生长因子治疗是治疗新生血管性年龄相关性黄斑变性(nAMD)的标准治疗方法。两种已获许可的药物——雷珠单抗和阿柏西普的剂量是通过临床试验确定的;然而,在常规临床实践中,这两种药物是否都按照推荐剂量使用尚不清楚。本研究使用药房理赔数据,调查了在治疗开始后 6 个月和 12 个月时,雷珠单抗的配药模式是否与阿柏西普的配药模式不同。
从澳大利亚 IMS AUS LRx 数据库中检索处方数据,以确定 2012 年 12 月 1 日至 2015 年 3 月 31 日期间有一个或多个雷珠单抗或阿柏西普理赔的 nAMD 患者,至少有 6 个月的随访。根据基线患者基于药物的疾病负担指数(MBDBI)评分调整雷珠单抗和阿柏西普的配药单位数。如果研究队列之间调整后平均差异的 95%置信区间(CI)下限在 1.00 单位或以下,则认为雷珠单抗与阿柏西普之间的配药单位数没有差异。
雷珠单抗(N=1235)和阿柏西普(N=959)队列的基线患者 MBDBI 评分相似。在第 6 个月和第 12 个月时,调整后的平均(标准差)配药单位数分别为 5.3(1.3)和 5.1(1.4)和 8.9(2.2)和 8.9(2.3)。在这两个时间点,调整后平均差异的 95%CI 均未超过 1.00 个单位:第 6 个月时调整后平均差异为 0.20 的 95%CI 为 0.09 至 0.32,第 12 个月时调整后平均差异为 0.04 的 95%CI 为-0.23 至 0.30。两个队列的平均(标准差)配药间隔相似:第 6 个月为 35.3(19.2)天和 36.8(20.0)天(调整后的平均差异-1.59 天;95%CI -2.51 至 -0.67 天),第 12 个月为 41.2(20.9)天和 41.6(20.4)天(调整后的平均差异-0.40 天;95%CI -1.70 至 0.91 天)。
在治疗的第一年,澳大利亚的药房以类似的方式配药雷珠单抗和阿柏西普。
诺华制药公司。