D'Ambruoso Lucia, Kahn Kathleen, Wagner Ryan G, Twine Rhian, Spies Barry, van der Merwe Maria, Gómez-Olivé F Xavier, Tollman Stephen, Byass Peter
Institute of Applied Health Sciences, University of Aberdeen, Scotland, UK.
Umeå Centre for Global Health Research, Umeå University, Umeå, Sweden.
Glob Health Res Policy. 2016 Jun 15;1:2. doi: 10.1186/s41256-016-0002-y. eCollection 2016.
Verbal autopsy (VA) is a health surveillance technique used in low and middle-income countries to establish medical causes of death (CODs) for people who die outside hospitals and/or without registration. By virtue of the deaths it investigates, VA is also an opportunity to examine social exclusion from access to health systems. The aims were to develop a system to collect and interpret information on social and health systems determinants of deaths investigated in VA.
A short set of questions on care pathways, circumstances and events at and around the time of death were developed and integrated into the WHO 2012 short form VA (SF-VA). Data were subsequently analysed from two census rounds in the Agincourt Health and Socio-Demographic Surveillance Site (HDSS), South Africa in 2012 and 2013 where the SF-VA had been applied. InterVA and descriptive analysis were used to calculate cause-specific mortality fractions (CSMFs), and to examine responses to the new indicators and whether and how they varied by medical CODs and age/sex sub-groups.
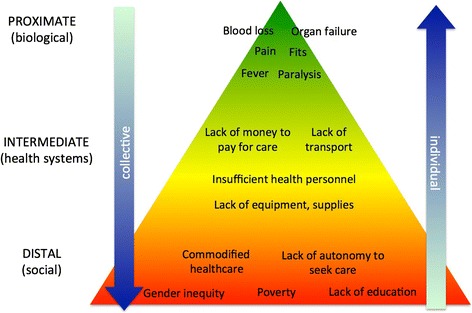
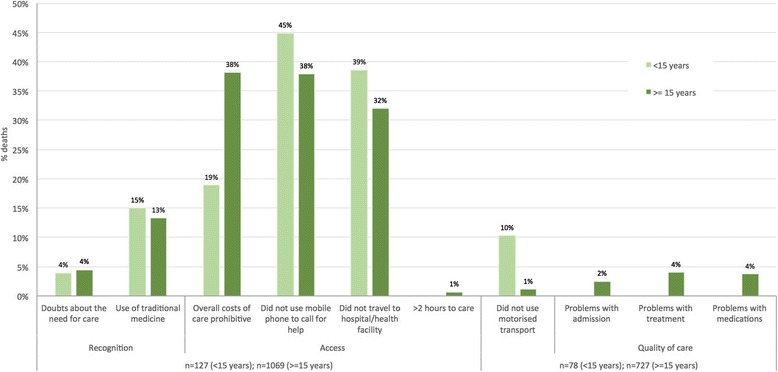
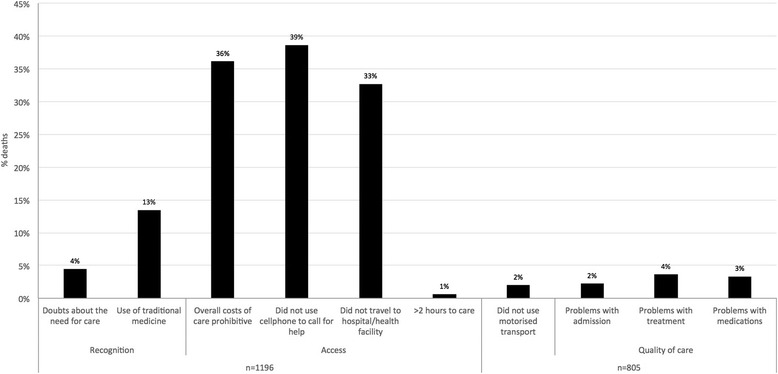
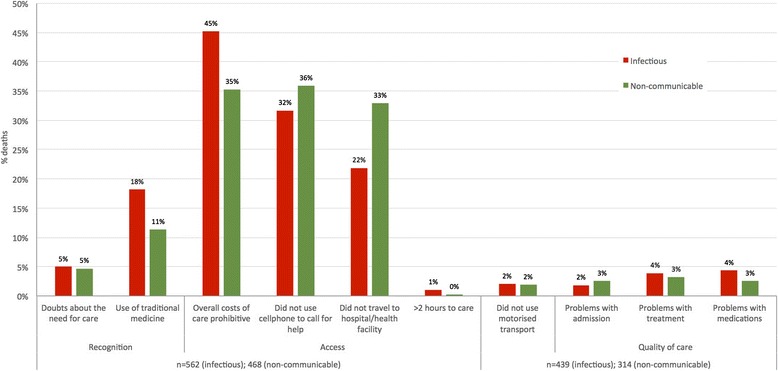
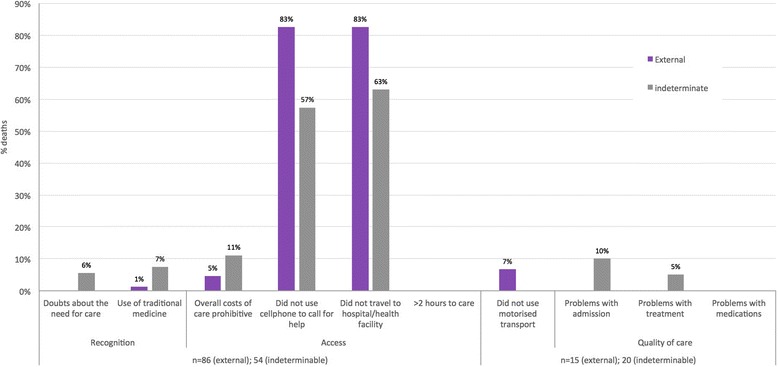
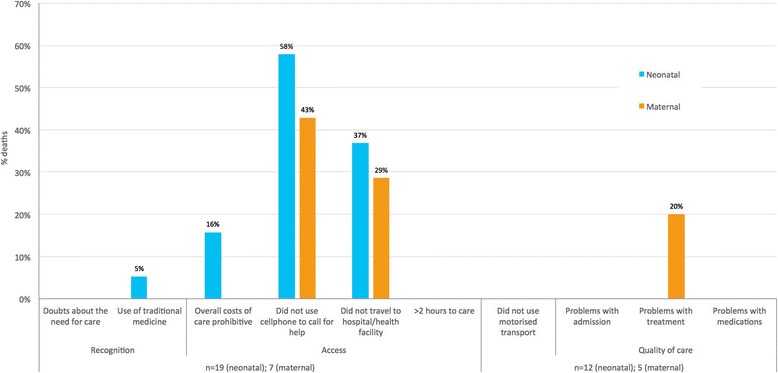
One thousand two hundred forty-nine deaths were recorded in the Agincourt HDSS censuses in 2012-13 of which 1,196 (96 %) had complete VA data. Infectious and non-communicable conditions accounted for the majority of deaths (47 % and 39 % respectively) with smaller proportions attributed to external, neonatal and maternal causes (5 %, 2 % and 1 % respectively). 5 % of deaths were of indeterminable cause. The new indicators revealed multiple problems with access to care at the time of death: 39 % of deaths did not call for help, 36 % found care unaffordable overall, and 33 % did not go to a facility. These problems were reported consistently across age and sex sub-groups. Acute conditions and younger age groups had fewer problems with overall costs but more with not calling for help or going to a facility. An illustrative health systems interpretation suggests extending and promoting existing provisions for transport and financial access in this setting.
Supplementing VA with questions on the circumstances of mortality provides complementary information to CSMFs relevant for health planning. Further contextualisation of the method and results are underway with health systems stakeholders to develop the interpretation sequence as part of a health policy and systems research approach.
口头尸检(VA)是一种在低收入和中等收入国家使用的健康监测技术,用于确定在医院外死亡和/或未登记死亡者的医学死因(COD)。鉴于其调查的死亡情况,VA也是一个审视因无法获得卫生系统服务而导致的社会排斥现象的契机。目的是开发一个系统,以收集和解读关于VA所调查死亡的社会和卫生系统决定因素的信息。
制定了一组关于死亡时的护理途径、情况和事件的简短问题,并将其纳入世界卫生组织2012年简版VA(SF-VA)。随后对2012年和2013年在南非阿金库尔健康与社会人口监测点(HDSS)进行的两轮人口普查数据进行了分析,这两轮普查应用了SF-VA。使用InterVA和描述性分析来计算特定病因死亡率(CSMF),并检查对新指标的回答,以及这些回答是否因医学死因和年龄/性别亚组而异,以及如何不同。
2012 - 2013年阿金库尔HDSS人口普查记录了1249例死亡,其中1196例(96%)有完整的VA数据。传染病和非传染性疾病占死亡的大多数(分别为47%和39%),较小比例归因于外部、新生儿和孕产妇原因(分别为5%、2%和1%)。5%的死亡原因无法确定。新指标揭示了死亡时获得护理存在的多个问题:39%的死亡没有呼救,36%的人总体上认为护理费用过高,33%的人没有前往医疗机构。这些问题在各年龄和性别亚组中均有一致报告。急性疾病和较年轻年龄组在总体费用方面问题较少,但在不呼救或不去医疗机构方面问题较多。一个示例性的卫生系统解读建议在这种情况下扩大和推广现有的交通和经济援助措施。
用关于死亡情况的问题补充VA,可为与卫生规划相关的CSMF提供补充信息。目前正在与卫生系统利益相关者进一步将该方法和结果置于具体背景中,以制定解读顺序,作为卫生政策和系统研究方法的一部分。