Williams Abimbola Onigbanjo, Makinde Olusesan Ayodeji, Ojo Mojisola
School of Public Health, Rutgers, The State University of New Jersey, 683 Hoes Lane, Piscataway, New Brunswick, 08854 NJ USA.
Ernest Mario School of Pharmacy, Rutgers, The State University of New Jersey, Piscataway, New Brunswick, NJ USA.
Glob Health Res Policy. 2016 Aug 2;1:10. doi: 10.1186/s41256-016-0010-y. eCollection 2016.
Multidrug drug resistant Tuberculosis (MDR-TB) and extensively drug resistant Tuberculosis (XDR-TB) have emerged as significant public health threats worldwide. This systematic review and meta-analysis aimed to investigate the effects of community-based treatment to traditional hospitalization in improving treatment success rates among MDR-TB and XDR-TB patients in the 27 MDR-TB High burden countries (HBC).
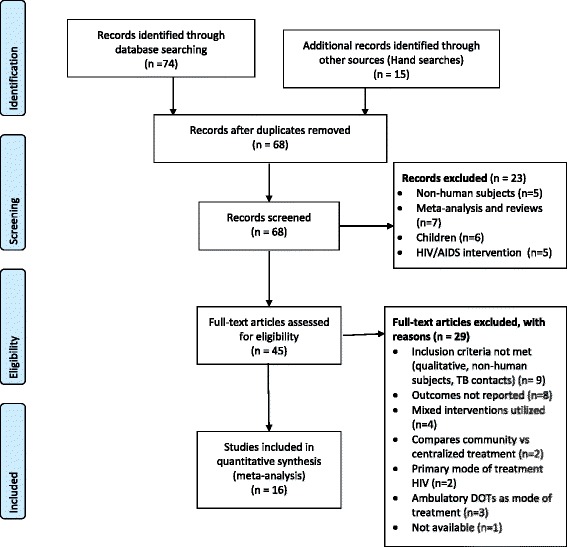
We searched PubMed, Cochrane, Lancet, Web of Science, International Journal of Tuberculosis and Lung Disease, and Centre for Reviews and Dissemination (CRD) for studies on community-based treatment and traditional hospitalization and MDR-TB and XDR-TB from the 27 MDR-TB HBC. Data on treatment success and failure rates were extracted from retrospective and prospective cohort studies, and a case control study. Sensitivity analysis, subgroup analyses, and meta-regression analysis were used to explore bias and potential sources of heterogeneity.
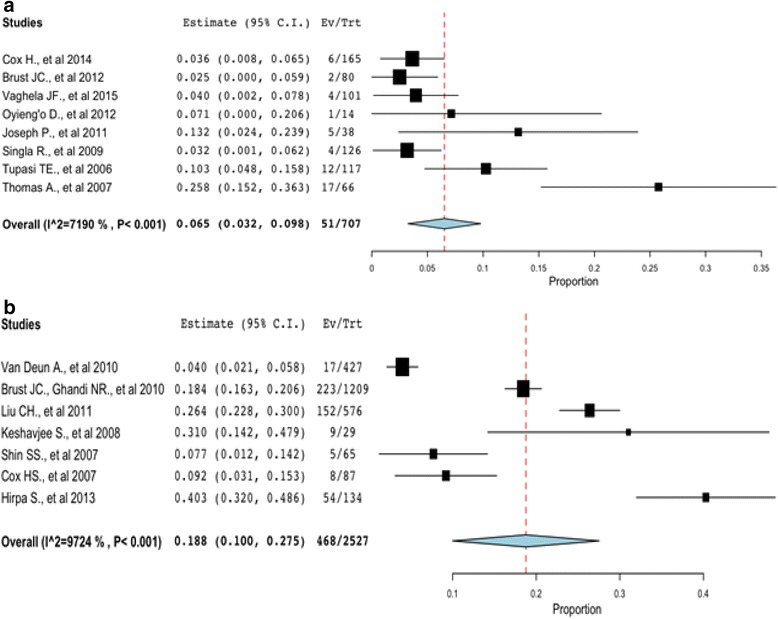
The final sample included 16 studies involving 3344 patients from nine countries; Bangladesh, China, Ethiopia, Kenya, India, South Africa, Philippines, Russia, and Uzbekistan. Based on a random-effects model, we observed a higher treatment success rate in community-based treatment (Point estimate = 0.68, 95 % CI: 0.59 to 0.76, < 0.01) compared to traditional hospitalization (Point estimate = 0.57, 95 % CI: 0.44 to 0.69, < 0.01). A lower treatment failure rate was observed in community-based treatment 7 % (Point estimate = 0.07, 95 % CI: 0.03 to 0.10; < 0.01) compared to traditional hospitalization (Point estimate = 0.188, 95 % CI: 0.10 to 0.28; < 0.01). In the subgroup analysis, studies without HIV co-infected patients, directly observed therapy short course-plus (DOTS-Plus) implemented throughout therapy, treatment duration > 18 months, and regimen with drugs >5 reported higher treatment success rate. In the meta-regression model, age of patients, adverse events, treatment duration, and lost to follow up explains some of the heterogeneity of treatment effects between studies.
Community-based management improved treatment outcomes. A mix of interventions with DOTS-Plus throughout therapy and treatment duration > 18 months as well as strategies in place for lost to follow up and adverse events should be considered in MDR-TB and XDR-TB interventions, as they influenced positively, treatment success.
耐多药结核病(MDR-TB)和广泛耐药结核病(XDR-TB)已成为全球重大的公共卫生威胁。本系统评价和荟萃分析旨在调查在27个耐多药结核病高负担国家(HBC)中,基于社区的治疗与传统住院治疗相比,在提高耐多药结核病和广泛耐药结核病患者治疗成功率方面的效果。
我们检索了PubMed、Cochrane、《柳叶刀》、科学网、《国际结核病和肺部疾病杂志》以及循证医学图书馆,以查找来自27个耐多药结核病高负担国家中关于基于社区的治疗、传统住院治疗以及耐多药结核病和广泛耐药结核病的研究。治疗成功和失败率的数据从回顾性和前瞻性队列研究以及一项病例对照研究中提取。采用敏感性分析、亚组分析和荟萃回归分析来探讨偏倚和潜在的异质性来源。
最终样本包括16项研究,涉及来自9个国家的3344名患者;孟加拉国、中国、埃塞俄比亚、肯尼亚、印度、南非、菲律宾、俄罗斯和乌兹别克斯坦。基于随机效应模型,我们观察到与传统住院治疗(点估计值 = 0.57,95%置信区间:0.44至0.69,P < 0.01)相比,基于社区的治疗具有更高的治疗成功率(点估计值 = 0.68,95%置信区间:0.59至0.76,P < 0.01)。与传统住院治疗(点估计值 = 0.188,95%置信区间:0.10至0.28,P < 0.01)相比,基于社区的治疗观察到更低的治疗失败率,为7%(点估计值 = 0.07,95%置信区间:0.03至0.10;P < 0.01)。在亚组分析中,没有合并感染艾滋病毒患者的研究、在整个治疗过程中实施直接观察下的短程治疗加强版(DOTS-Plus)、治疗持续时间>18个月以及使用超过5种药物的治疗方案报告了更高的治疗成功率。在荟萃回归模型中,患者年龄、不良事件、治疗持续时间和失访情况解释了各研究间治疗效果异质性的部分原因。
基于社区的管理改善了治疗结果。在耐多药结核病和广泛耐药结核病干预措施中,应考虑在整个治疗过程中采用DOTS-Plus的综合干预措施、治疗持续时间>18个月以及针对失访和不良事件的策略,因为它们对治疗成功产生了积极影响。