Department of Microbiology and Immunology, University of Western Ontario, 1151 Richmond St., Dental Sciences Bldg., Rm 3014, London, Ontario, N6A 5C1, Canada.
Division of Infectious Diseases, Department of Medicine, Case Western Reserve University, Cleveland, OH, USA.
Infect Dis Poverty. 2017 Dec 4;6(1):163. doi: 10.1186/s40249-017-0377-0.
Thymidine analogs, namely AZT (Zidovudine or Retrovir™) and d4T (Stavudine or Zerit™) are antiretroviral drugs still employed in over 75% of first line combination antiretroviral therapy (cART) in Kampala, Uganda despite aversion to prescribing these drugs for cART in high income countries due in part to adverse events. For this study, we explored how the continued use of these thymidine analogs in cART could impact emergence of drug resistance and impact on future treatment success in Uganda, a low-income country.
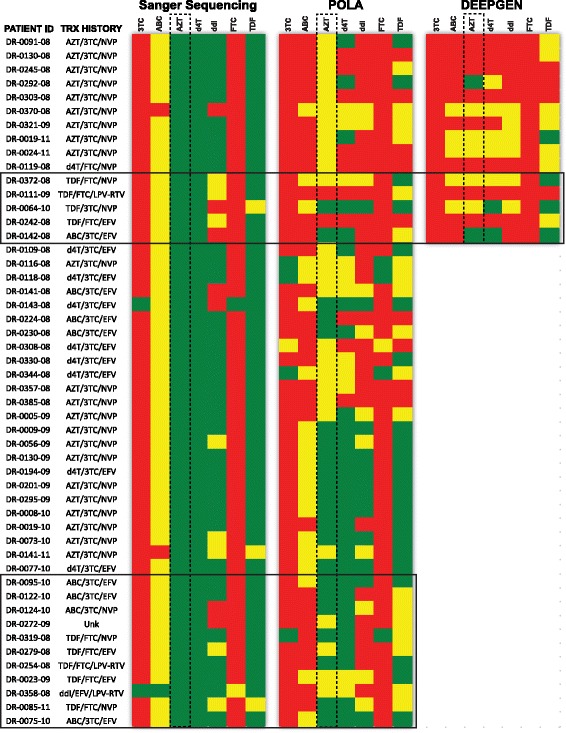
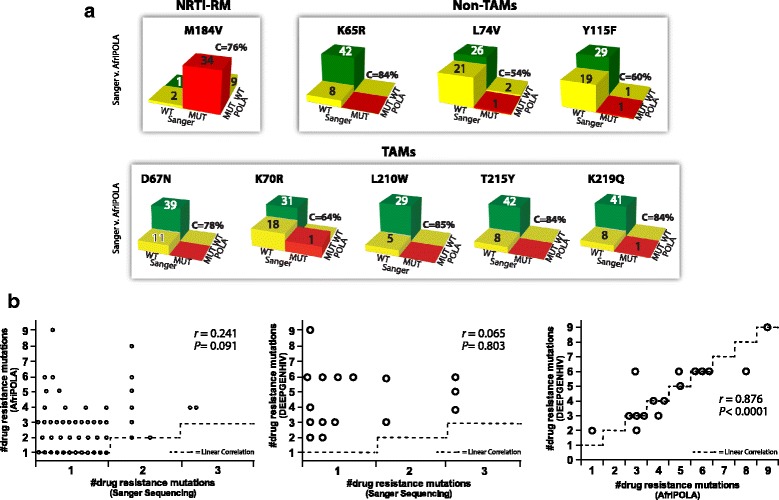
We examined the drug resistance genotypes by Sanger sequencing of 262 HIV-infected patients failing a first line combined antiretroviral treatment containing either AZT or d4T, which represents approximately 5% of the patients at the Joint Clinical Research Center receiving a AZT or d4T containing treatment. Next generation sequencing (DEEPGEN™HIV) and multiplex oligonucleotide ligation assays (AfriPOLA) were then performed on a subset of patient samples to detect low frequency drug resistant mutations. CD4 cell counts, viral RNA loads, and treatment changes were analyzed in a cohort of treatment success and failures.
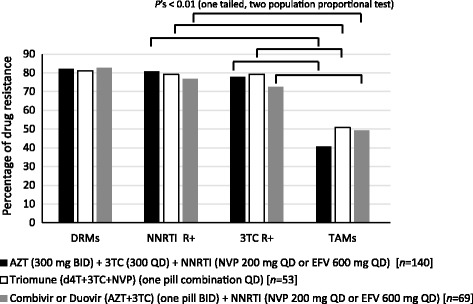
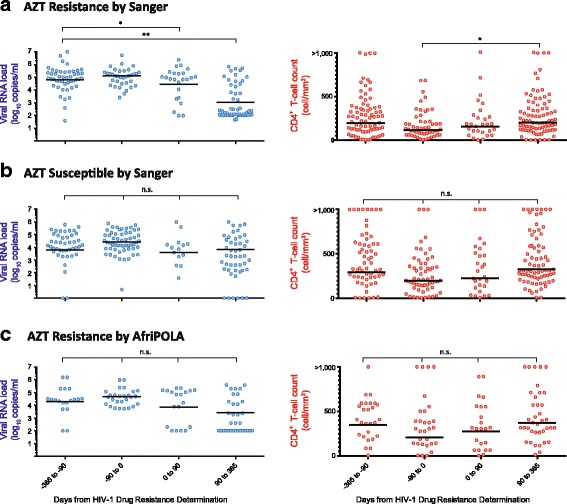
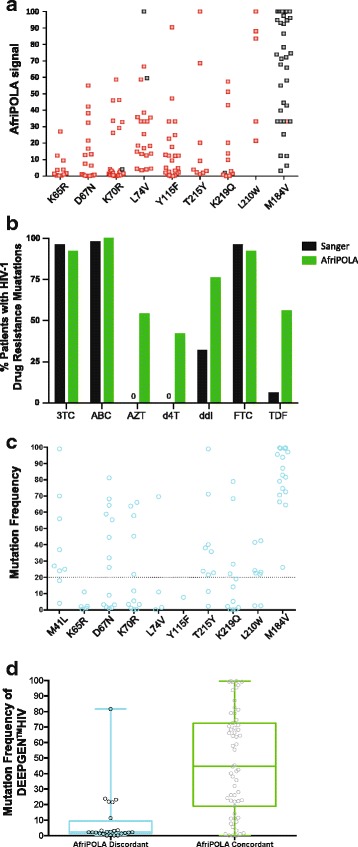
Over 80% of patients failing first line AZT/d4T-containing cART had predicted drug resistance to 3TC (Lamivudine) and non-nucleoside RT inhibitors (NNRTIs) in the treatment regimen but only 45% had resistance AZT/d4T associated resistance mutations (TAMs). TAMs were however detected at low frequency within the patients HIV quasispecies (1-20%) in 21 of 34 individuals who were failing first-line AZT-containing cART and lacked TAMs by Sanger. Due to lack of TAMs by Sanger, AZT was typically maintained in second-line therapies and these patients had a low frequency of subsequent virologic success.
Our findings suggest that continued use of AZT and d4T in first-line treatment in low-to-middle income countries may lead to misdiagnosis of HIV-1 drug resistance and possibly enhance a succession of second- and third-line treatment failures.
胸腺嘧啶核苷类似物,即 AZT(齐多夫定或立妥威)和 d4T(司他夫定或赛瑞特),是抗逆转录病毒药物,尽管在高收入国家由于不良反应而避免将这些药物用于 cART,但在乌干达坎帕拉,它们仍在超过 75%的一线联合抗逆转录病毒疗法(cART)中使用。对于这项研究,我们探讨了在低收入国家乌干达,cART 中继续使用这些胸苷类似物如何影响耐药性的出现以及对未来治疗成功的影响。
我们通过对 262 名在一线联合抗逆转录病毒治疗中使用 AZT 或 d4T 失败的 HIV 感染患者的耐药基因型进行 Sanger 测序来进行检查,这代表在接受 AZT 或 d4T 治疗的联合临床研究中心患者中,约有 5%的患者出现这种情况。然后,对部分患者样本进行下一代测序(DEEPGEN™HIV)和多重寡核苷酸连接分析(AfriPOLA),以检测低频耐药突变。对治疗成功和失败的患者队列进行 CD4 细胞计数、病毒 RNA 载量和治疗变化分析。
超过 80%的一线 AZT/d4T 联合 cART 治疗失败的患者在治疗方案中对 3TC(拉米夫定)和非核苷逆转录酶抑制剂(NNRTIs)有预测耐药性,但只有 45%的患者有 AZT/d4T 相关耐药突变(TAMs)。然而,在 34 名一线 AZT 联合 cART 治疗失败且 Sanger 未检测到 TAMs 的患者中,21 名患者的 HIV 准种中检测到低频率的 TAMs(1-20%)。由于 Sanger 未检测到 TAMs,AZT 通常保留在二线治疗中,这些患者随后的病毒学成功率较低。
我们的发现表明,在中低收入国家一线治疗中继续使用 AZT 和 d4T 可能导致 HIV-1 耐药性的误诊,并可能增加二线和三线治疗失败的后续可能性。