Rhee Soo-Yon, Blanco Jose Luis, Jordan Michael R, Taylor Jonathan, Lemey Philippe, Varghese Vici, Hamers Raph L, Bertagnolio Silvia, Rinke de Wit Tobias F, Aghokeng Avelin F, Albert Jan, Avi Radko, Avila-Rios Santiago, Bessong Pascal O, Brooks James I, Boucher Charles A B, Brumme Zabrina L, Busch Michael P, Bussmann Hermann, Chaix Marie-Laure, Chin Bum Sik, D'Aquin Toni T, De Gascun Cillian F, Derache Anne, Descamps Diane, Deshpande Alaka K, Djoko Cyrille F, Eshleman Susan H, Fleury Herve, Frange Pierre, Fujisaki Seiichiro, Harrigan P Richard, Hattori Junko, Holguin Africa, Hunt Gillian M, Ichimura Hiroshi, Kaleebu Pontiano, Katzenstein David, Kiertiburanakul Sasisopin, Kim Jerome H, Kim Sung Soon, Li Yanpeng, Lutsar Irja, Morris Lynn, Ndembi Nicaise, Ng Kee Peng, Paranjape Ramesh S, Peeters Martine, Poljak Mario, Price Matt A, Ragonnet-Cronin Manon L, Reyes-Terán Gustavo, Rolland Morgane, Sirivichayakul Sunee, Smith Davey M, Soares Marcelo A, Soriano Vincent V, Ssemwanga Deogratius, Stanojevic Maja, Stefani Mariane A, Sugiura Wataru, Sungkanuparph Somnuek, Tanuri Amilcar, Tee Kok Keng, Truong Hong-Ha M, van de Vijver David A M C, Vidal Nicole, Yang Chunfu, Yang Rongge, Yebra Gonzalo, Ioannidis John P A, Vandamme Anne-Mieke, Shafer Robert W
Department of Medicine, Stanford University, Stanford, California, United States of America. Leuven—University of Leuven, Department of Microbiology and Immunology, Rega Institute for Medical Research, Clinical and Epidemiological Virology, Leuven, Belgium.
Hospital Clinic Universitari-Institut d'Investigacions Biomèdiques August Pi i Sunyer, University of Barcelona, Barcelona, Spain.
PLoS Med. 2015 Apr 7;12(4):e1001810. doi: 10.1371/journal.pmed.1001810. eCollection 2015 Apr.
Regional and subtype-specific mutational patterns of HIV-1 transmitted drug resistance (TDR) are essential for informing first-line antiretroviral (ARV) therapy guidelines and designing diagnostic assays for use in regions where standard genotypic resistance testing is not affordable. We sought to understand the molecular epidemiology of TDR and to identify the HIV-1 drug-resistance mutations responsible for TDR in different regions and virus subtypes.
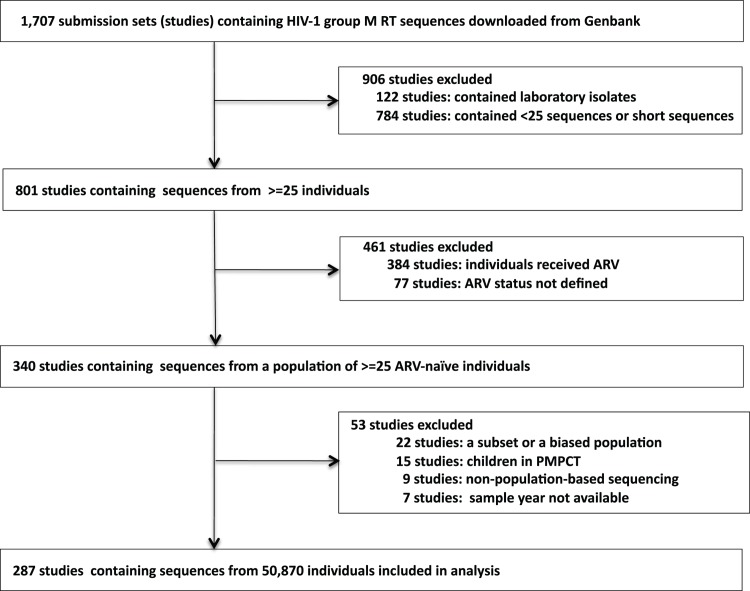
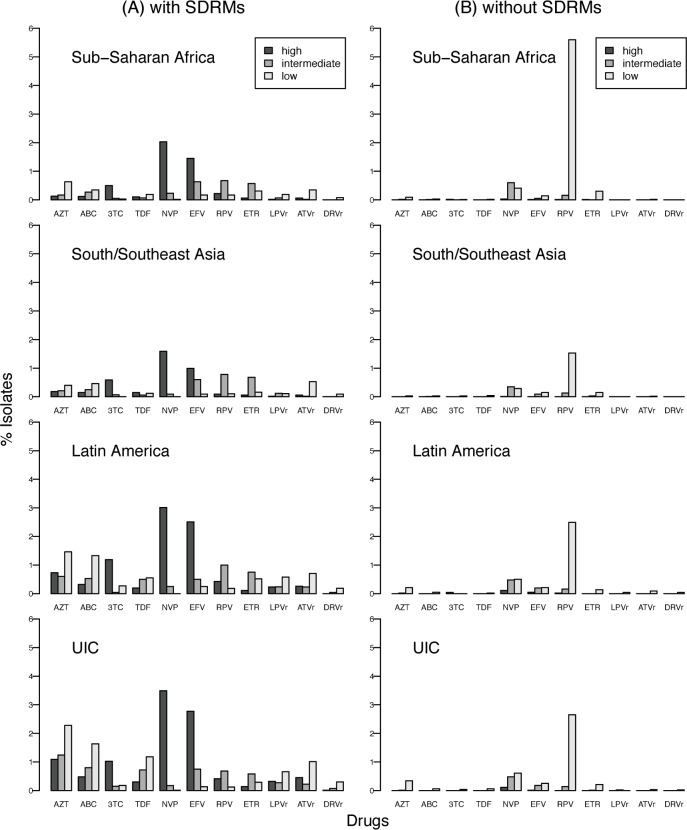
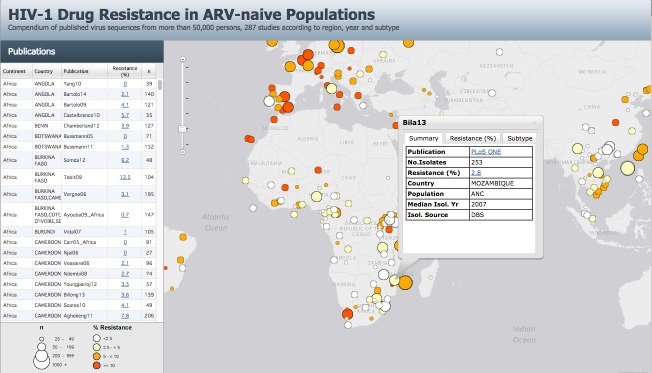
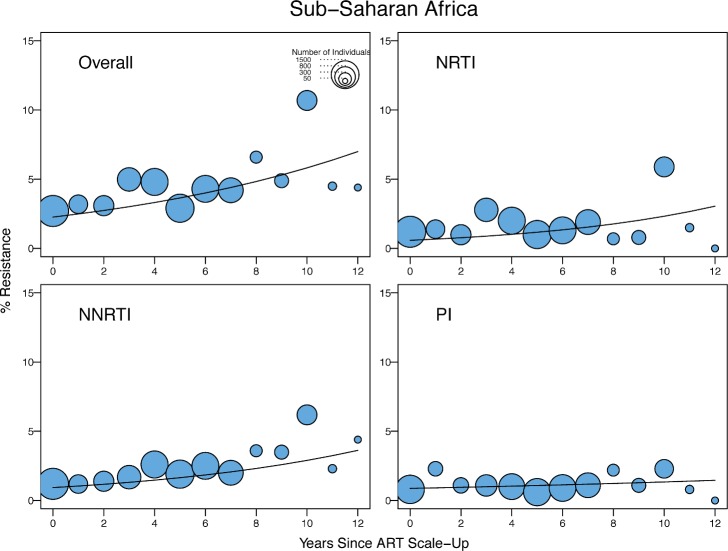
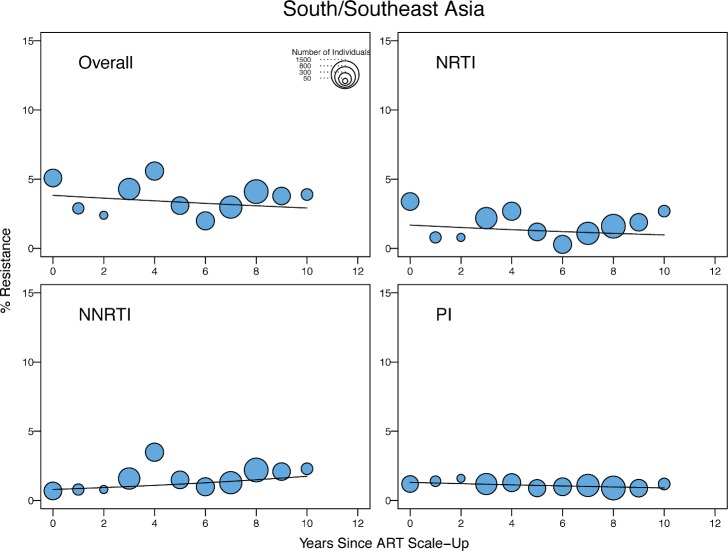
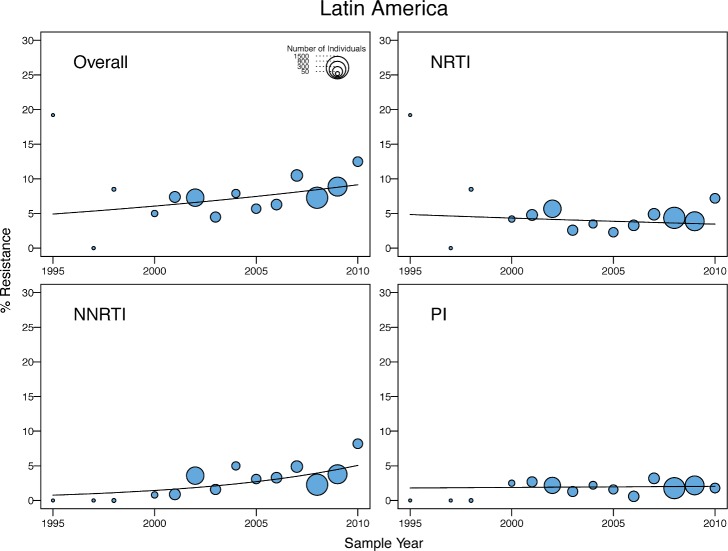
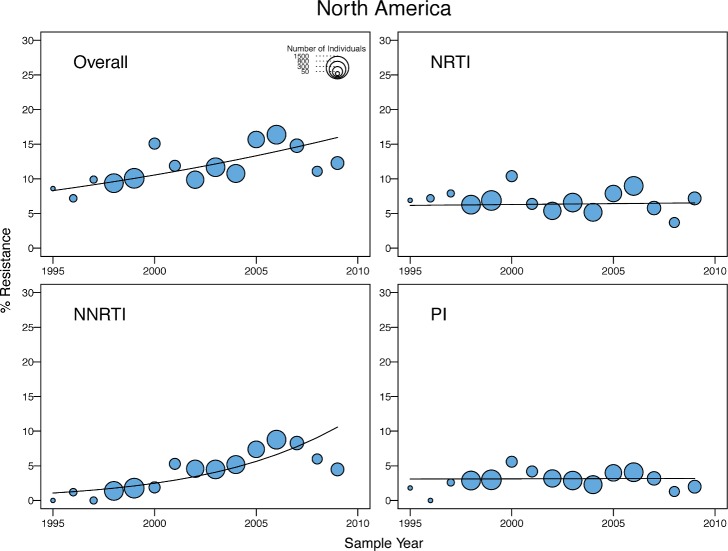
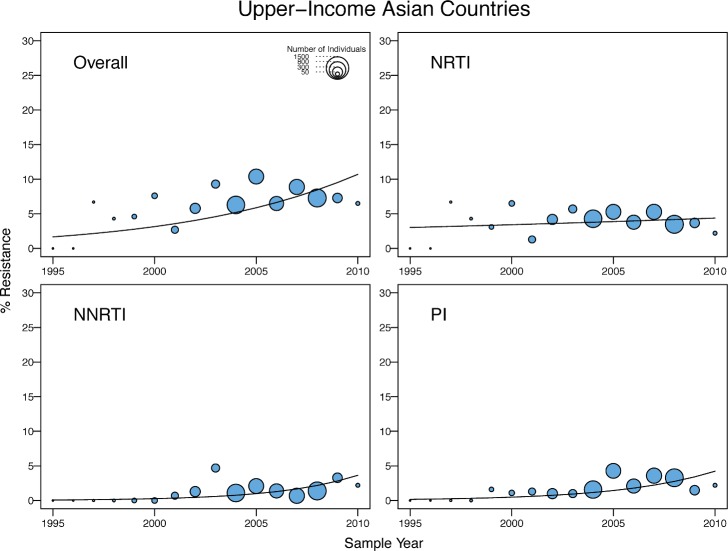
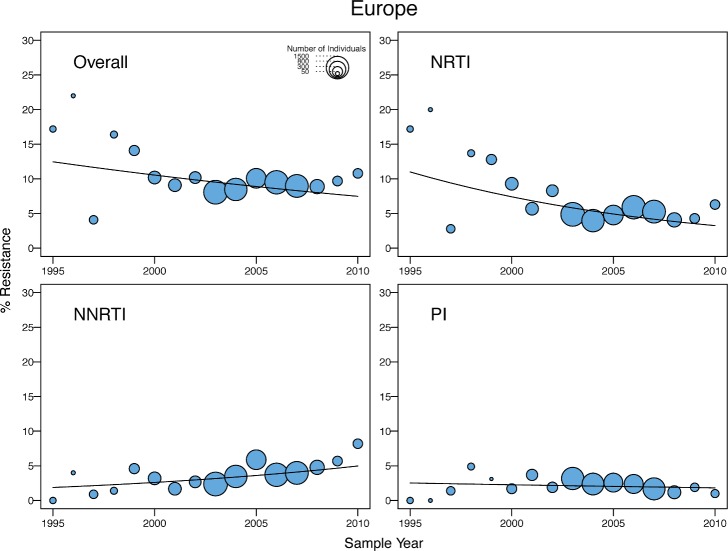
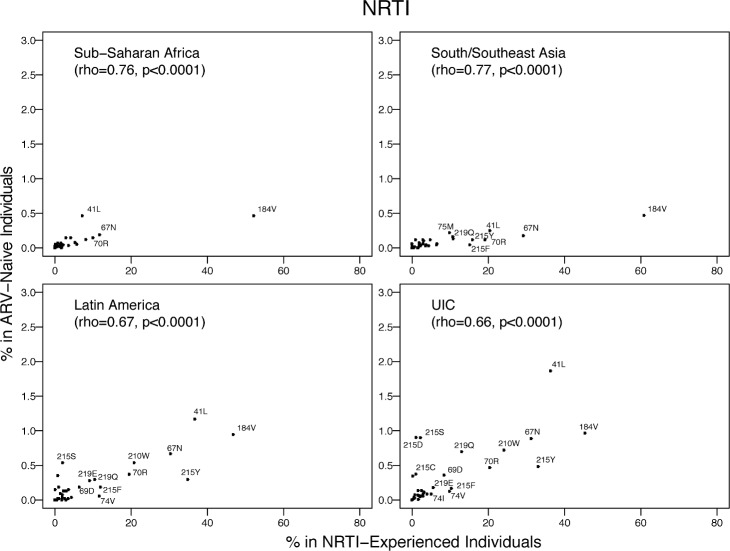
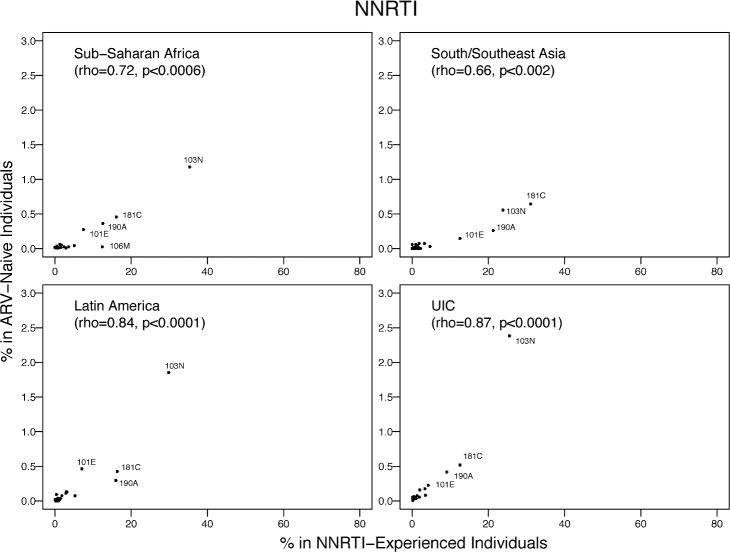
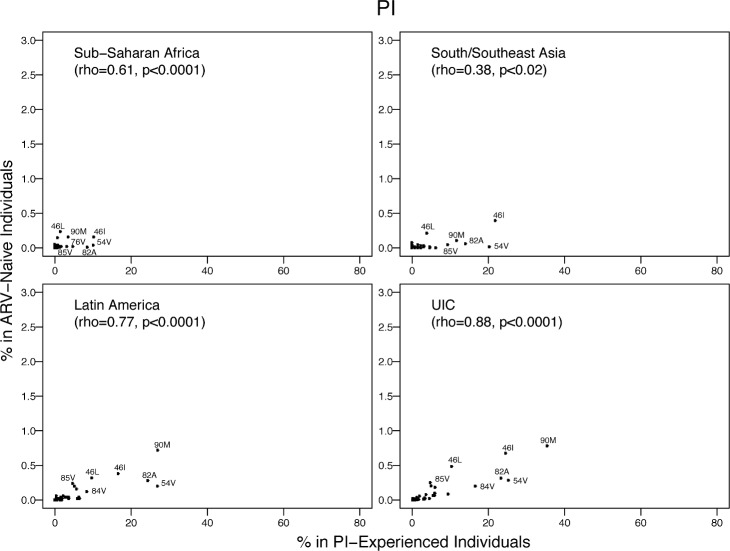
We reviewed all GenBank submissions of HIV-1 reverse transcriptase sequences with or without protease and identified 287 studies published between March 1, 2000, and December 31, 2013, with more than 25 recently or chronically infected ARV-naïve individuals. These studies comprised 50,870 individuals from 111 countries. Each set of study sequences was analyzed for phylogenetic clustering and the presence of 93 surveillance drug-resistance mutations (SDRMs). The median overall TDR prevalence in sub-Saharan Africa (SSA), south/southeast Asia (SSEA), upper-income Asian countries, Latin America/Caribbean, Europe, and North America was 2.8%, 2.9%, 5.6%, 7.6%, 9.4%, and 11.5%, respectively. In SSA, there was a yearly 1.09-fold (95% CI: 1.05-1.14) increase in odds of TDR since national ARV scale-up attributable to an increase in non-nucleoside reverse transcriptase inhibitor (NNRTI) resistance. The odds of NNRTI-associated TDR also increased in Latin America/Caribbean (odds ratio [OR] = 1.16; 95% CI: 1.06-1.25), North America (OR = 1.19; 95% CI: 1.12-1.26), Europe (OR = 1.07; 95% CI: 1.01-1.13), and upper-income Asian countries (OR = 1.33; 95% CI: 1.12-1.55). In SSEA, there was no significant change in the odds of TDR since national ARV scale-up (OR = 0.97; 95% CI: 0.92-1.02). An analysis limited to sequences with mixtures at less than 0.5% of their nucleotide positions—a proxy for recent infection—yielded trends comparable to those obtained using the complete dataset. Four NNRTI SDRMs—K101E, K103N, Y181C, and G190A—accounted for >80% of NNRTI-associated TDR in all regions and subtypes. Sixteen nucleoside reverse transcriptase inhibitor (NRTI) SDRMs accounted for >69% of NRTI-associated TDR in all regions and subtypes. In SSA and SSEA, 89% of NNRTI SDRMs were associated with high-level resistance to nevirapine or efavirenz, whereas only 27% of NRTI SDRMs were associated with high-level resistance to zidovudine, lamivudine, tenofovir, or abacavir. Of 763 viruses with TDR in SSA and SSEA, 725 (95%) were genetically dissimilar; 38 (5%) formed 19 sequence pairs. Inherent limitations of this study are that some cohorts may not represent the broader regional population and that studies were heterogeneous with respect to duration of infection prior to sampling.
Most TDR strains in SSA and SSEA arose independently, suggesting that ARV regimens with a high genetic barrier to resistance combined with improved patient adherence may mitigate TDR increases by reducing the generation of new ARV-resistant strains. A small number of NNRTI-resistance mutations were responsible for most cases of high-level resistance, suggesting that inexpensive point-mutation assays to detect these mutations may be useful for pre-therapy screening in regions with high levels of TDR. In the context of a public health approach to ARV therapy, a reliable point-of-care genotypic resistance test could identify which patients should receive standard first-line therapy and which should receive a protease-inhibitor-containing regimen.
HIV-1传播耐药性(TDR)的区域和亚型特异性突变模式对于制定一线抗逆转录病毒(ARV)治疗指南以及设计用于标准基因型耐药性检测难以负担地区的诊断检测至关重要。我们试图了解TDR的分子流行病学,并确定不同地区和病毒亚型中导致TDR的HIV-1耐药性突变。
我们回顾了GenBank中所有提交的HIV-1逆转录酶序列(有或无蛋白酶序列),并确定了2000年3月1日至2013年12月31日期间发表的287项研究,这些研究涉及25名以上近期或慢性感染且未接受过抗逆转录病毒治疗的个体。这些研究涵盖了来自111个国家的50,870名个体。对每组研究序列进行系统发育聚类分析,并检测93种监测耐药性突变(SDRM)的存在情况。撒哈拉以南非洲(SSA)、南亚/东南亚(SSEA)、高收入亚洲国家、拉丁美洲/加勒比地区、欧洲和北美的总体TDR患病率中位数分别为2.8%、2.9%、5.6%、7.6%、9.4%和11.5%。在SSA,自国家扩大抗逆转录病毒治疗规模以来,由于非核苷类逆转录酶抑制剂(NNRTI)耐药性增加,TDR的发生几率每年增加1.09倍(95%CI:1.05 - 1.14)。拉丁美洲/加勒比地区(优势比[OR]=1.16;95%CI:1.06 - 1.25)、北美(OR = 1.19;95%CI:1.12 - 1.26)、欧洲(OR = 1.07;95%CI:1.01 - 1.13)和高收入亚洲国家(OR = 1.33;95%CI:1.12 - 1.55)的NNRTI相关TDR发生几率也有所增加。在SSEA,自国家扩大抗逆转录病毒治疗规模以来,TDR的发生几率没有显著变化(OR = 0.97;95%CI:0.92 - 1.02)。一项仅限于核苷酸位置混合比例低于0.5%(代表近期感染)的序列分析得出的趋势与使用完整数据集得到的趋势相似。四种NNRTI SDRM——K101E、K103N、Y181C和G190A——在所有地区和亚型中占NNRTI相关TDR的比例超过80%。16种核苷类逆转录酶抑制剂(NRTI)SDRM在所有地区和亚型中占NRTI相关TDR的比例超过69%。在SSA和SSEA,89%的NNRTI SDRM与对奈韦拉平或依非韦伦的高水平耐药相关,而只有27%的NRTI SDRM与对齐多夫定、拉米夫定、替诺福韦或阿巴卡韦的高水平耐药相关。在SSA和SSEA的763株具有TDR的病毒中,725株(95%)在基因上不相似;38株(5%)形成了19个序列对。本研究的固有局限性在于,一些队列可能不代表更广泛的区域人群,且研究在采样前的感染持续时间方面存在异质性。
SSA和SSEA中的大多数TDR毒株是独立出现的,这表明具有高耐药基因屏障的抗逆转录病毒治疗方案与改善患者依从性相结合,可能通过减少新的抗逆转录病毒耐药毒株的产生来减轻TDR的增加。少数NNRTI耐药性突变导致了大多数高水平耐药病例,这表明用于检测这些突变的廉价点突变检测方法可能有助于在TDR水平较高的地区进行治疗前筛查。在抗逆转录病毒治疗的公共卫生方法背景下,可靠的即时基因型耐药性检测可以确定哪些患者应接受标准一线治疗,哪些患者应接受含蛋白酶抑制剂的治疗方案。