Posporis Christoforos, Grau-Roma Llorenç, Travetti Olga, Oliveira Maria, Polledo Laura, Wessmann Annette
Department of Neurology / Neurosurgery, Pride Veterinary Centre, Derby, UK.
School of Veterinary Medicine and Science, University of Nottingham, UK.
JFMS Open Rep. 2017 Nov 23;3(2):2055116917742812. doi: 10.1177/2055116917742812. eCollection 2017 Jul-Dec.
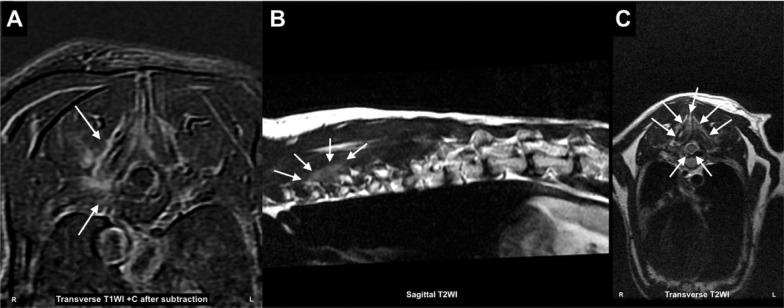
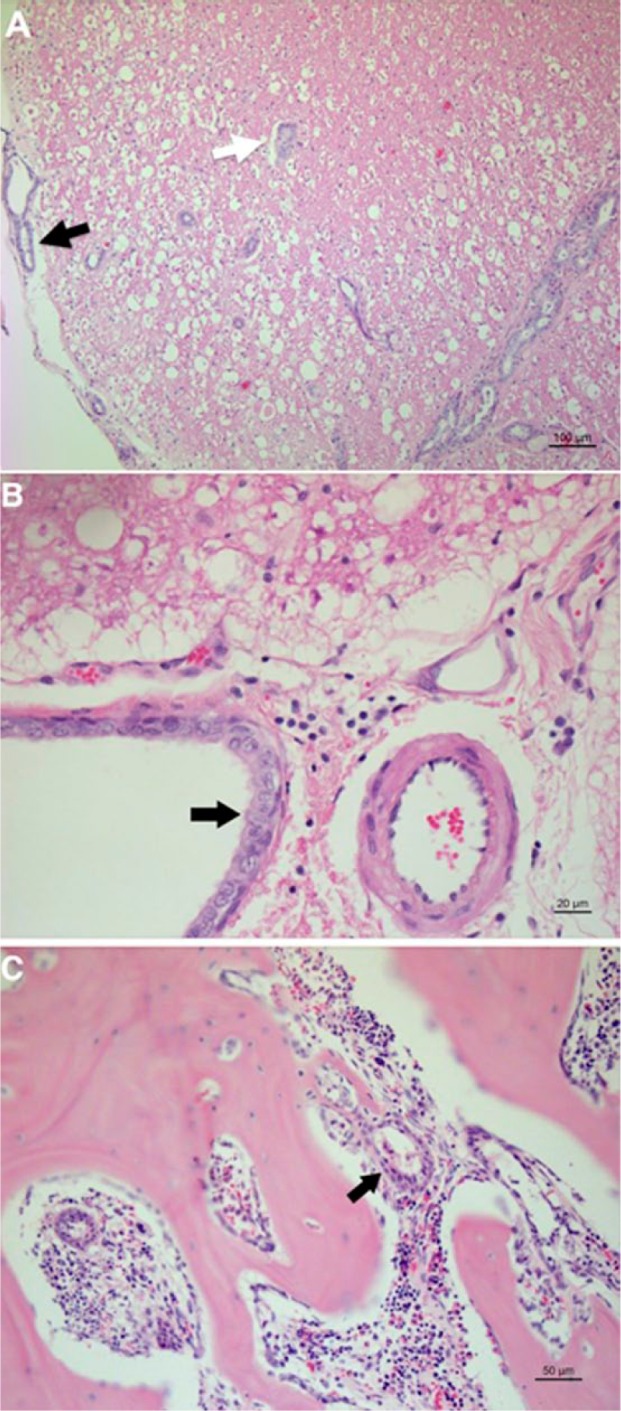
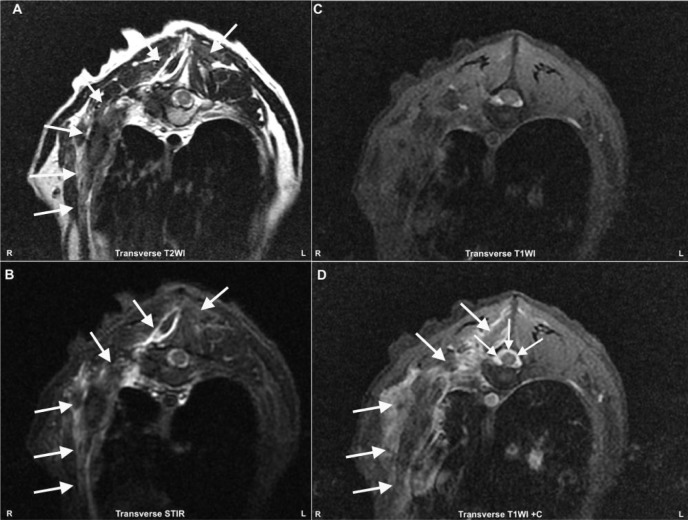
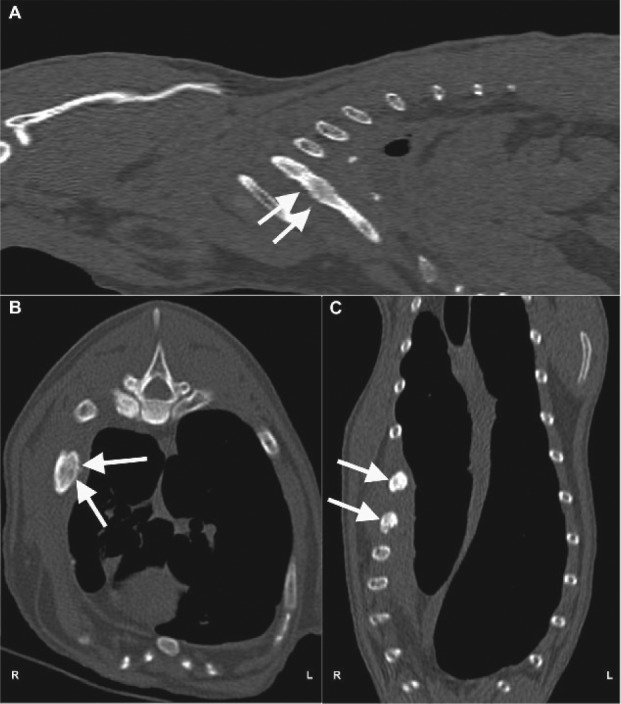
A 12-year-old domestic shorthair cat was presented with acute non-painful hindlimb proprioceptive ataxia localising to T3-L3 spinal cord segments. MRI revealed paravertebral muscular hyperintensity on T2-weighted images at the level of T7-T8 vertebrae. The cat improved on conservative management but deteriorated 3 months later. Repeated MRI showed meningeal enhancement at the same level and hyperintensity of the paravertebral musculature extending to the right thoracic wall and pleural space on short tau inversion recovery images. Thoracic CT showed mineralised lesions of the right lung, restricted pleural effusion and expansile bone lesions affecting multiple ribs. The cat had been treated for pyothorax 5 years earlier but manifested no current respiratory signs. Cerebrospinal fluid (CSF) examination showed lymphocytic pleocytosis but no neoplastic cells. Biopsy of the affected muscles and cytology of the lung and pleural lesions suggested a malignant epithelial cell tumour. Post-mortem examination confirmed a pulmonary adenocarcinoma locally infiltrating the thoracic wall, T7-T8 vertebrae and the spinal cord white matter. Meningeal carcinomatosis was detected with neoplastic cells invading the ventral median fissure of the spinal cord. No metastases were observed in other organs, indicating that neoplastic cells reached the spinal cord by direct extension.
Spinal meningeal carcinomatosis has not been reported in dogs or cats with extraneural tumours but is a well-recognised condition in humans. A metastatic cause of meningeal enhancement should be considered in patients with neurological signs of unknown origin. Imaging findings and CSF results can be non-specific.
一只12岁的家养短毛猫出现急性无痛性后肢本体感觉共济失调,定位在T3 - L3脊髓节段。MRI显示在T7 - T8椎体水平的T2加权图像上椎旁肌肉信号增强。这只猫在保守治疗后有所改善,但3个月后病情恶化。重复MRI显示同一水平的脑膜强化,并且在短tau反转恢复图像上椎旁肌肉组织信号增强延伸至右胸壁和胸膜腔。胸部CT显示右肺有矿化病变、局限性胸腔积液以及影响多根肋骨的膨胀性骨病变。这只猫5年前曾因脓胸接受治疗,但目前没有呼吸症状。脑脊液(CSF)检查显示淋巴细胞增多,但无肿瘤细胞。对受影响肌肉的活检以及肺部和胸膜病变的细胞学检查提示为恶性上皮细胞瘤。尸检证实为肺腺癌,局部浸润胸壁、T7 - T8椎体和脊髓白质。检测到脑膜癌病,肿瘤细胞侵入脊髓腹侧正中裂。在其他器官未观察到转移,表明肿瘤细胞是通过直接蔓延到达脊髓的。
脊髓脑膜癌病在患有神经外肿瘤的犬猫中尚未见报道,但在人类中是一种公认的疾病。对于病因不明的神经系统症状患者,应考虑脑膜强化的转移原因。影像学表现和脑脊液结果可能不具有特异性。