Rodgers Brian, Lin Jim, Staecker Hinrich
Michigan Ear Institute, Farmington Hills, MI 48334, USA.
Department of Otolaryngology Head and Neck Surgery, University of Kansas School of Medicine, KS 66061, USA.
World J Otorhinolaryngol Head Neck Surg. 2016 Dec 4;2(3):161-167. doi: 10.1016/j.wjorl.2016.11.001. eCollection 2016 Sep.
To compare and contrast our experience with middle cranial fossa approach (MFR) and transmastoid approach with capping of the dehiscence (TMR) of superior semicircular canal dehiscence and to determine guidelines to help guide management of these patients.
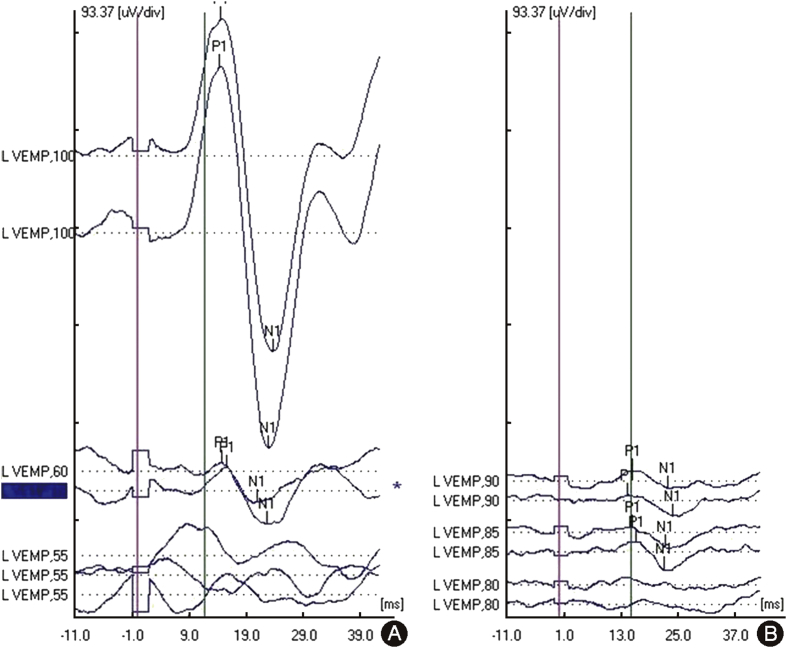
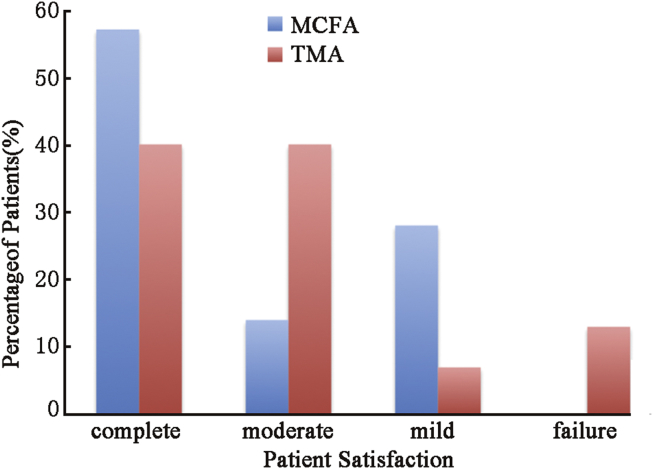
All patients from 2005 to 2014 with symptomatic superior semicircular canal dehiscence syndrome with dehiscence demonstrated on CT scan of the temporal bone who underwent surgical repair and had a minimum 3 months of follow up. Surgical repair via the MFR or TMR, preoperative CT temporal bone, preoperative, and postoperative cervical vestibular evoked myogenic potential (cVEMP) testing and anterior canal video head thrust testing (vHIT). Success of repair was stratified as complete success, moderate success, mild success, or failure based on resolution of all symptoms, the chief complaint, some symptoms, or no improvement, respectively.
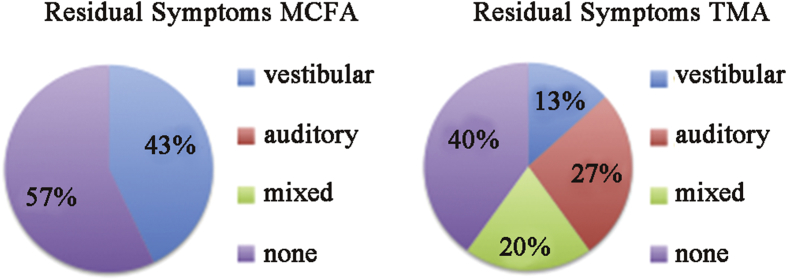
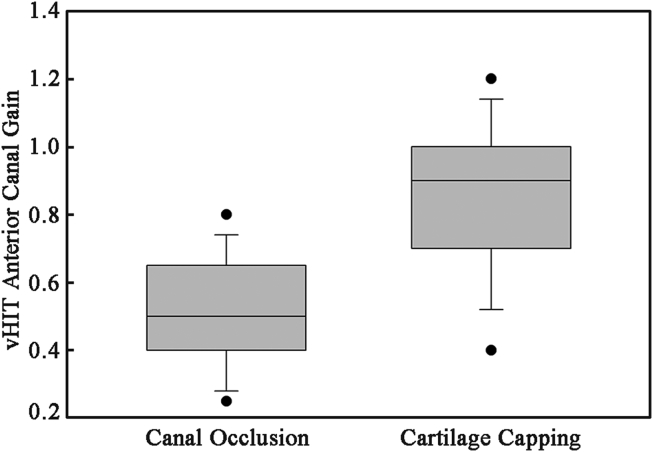
A total of 29 ears in 27 patients underwent surgical repair of canal dehiscence. Complete or moderate success was seen in 71% of the MFR group compared to 80% of the TMR group. There were zero failures with the MFR group and no major intracranial complications. There were 2 failures out of 15 ears that underwent the TMR. Residual symptoms were most commonly vertigo or disequilibrium in the MFR and aural fullness or autophony in the TMR groups, respectively. MFR hospital stay was approximately 2 days longer. Average cVEMP threshold shifted 18 dB with surgical correction in the MFR group. A 29 dB average shift was seen in the TMR group. The MFR group had a significant reduction in their anterior canal gain compared to the TMR group.
TMR is a less invasive alternative to MFR. However, in our series, we have not seen any intracranial complications (aphasia, stroke, seizures, etc.) in our MFR patients. Interestingly, vestibular symptoms were better addressed than audiological symptoms by the TMR suggesting its usefulness as a less invasive option for patients with primarily vestibular complaints. Residual auditory symptoms in TMR patients may be due to the flow of acoustic energy from the superior canal to the mastoid cavity through an incompletely sealed third window.
比较和对比我们采用中颅窝入路(MFR)和经乳突入路并封闭上半规管裂孔(TMR)治疗上半规管裂综合征的经验,并确定有助于指导这些患者治疗的指南。
纳入2005年至2014年间所有颞骨CT扫描显示有症状性上半规管裂综合征且有裂孔、接受手术修复并至少随访3个月的患者。通过MFR或TMR进行手术修复,术前行颞骨CT、术前和术后进行颈前庭诱发肌源性电位(cVEMP)测试以及前半规管视频头脉冲测试(vHIT)。根据所有症状、主要诉求、部分症状或无改善的缓解情况,将修复成功分为完全成功、中度成功、轻度成功或失败。
27例患者共29耳接受了半规管裂孔的手术修复。MFR组71%的患者获得完全或中度成功,而TMR组为80%。MFR组无一例失败,也无重大颅内并发症。15耳接受TMR手术的患者中有2例失败。MFR组残留症状最常见的是眩晕或平衡失调,TMR组则分别是耳闷或自听过强。MFR组住院时间约长2天。MFR组手术矫正后平均cVEMP阈值偏移18dB。TMR组平均偏移29dB。与TMR组相比,MFR组前半规管增益显著降低。
TMR是一种比MFR侵入性更小的替代方法。然而,在我们的系列研究中,MFR患者未出现任何颅内并发症(失语、中风、癫痫等)。有趣的是,TMR对前庭症状的改善优于听觉症状,这表明它对于主要有前庭症状的患者是一种侵入性较小的有用选择。TMR患者残留听觉症状可能是由于声能通过未完全封闭的第三窗从上半规管流向乳突腔。