Gizaw Muluken, Addissie Adamu, Getachew Sefonias, Ayele Wondimu, Mitiku Israel, Moelle Ulrike, Yusuf Tigist, Begoihn Mathias, Assefa Mathewos, Jemal Ahmedin, Kantelhardt Eva Johanna
Institute of Medical Epidemiology, Biostatistics and Informatics, Martin-Luther-University, Halle (Saale), Germany.
Department of Preventive Medicine, School of Public Health, Addis Ababa University, Addis Ababa, Ethiopia.
Infect Agent Cancer. 2017 Nov 29;12:61. doi: 10.1186/s13027-017-0171-4. eCollection 2017.
Women infected with Human Immune Deficiency Virus (HIV) are assumed to be at higher risk of developing Cervical Cancer (CC). This is due to a rapid progression of pre-invasive to invasive lesions. However, evidences suggest, due to the availability of antiretroviral therapy (ART) and care services; an improved survival and treatment outcome of CC patients (CCPs) with HIV infection is expected.
The aim of this study is to examine the clinical characteristics and survival of of CCPs registered at the radiotherapy center of Tikur Anbessa Specialized Hospital (TASH), Addis Ababa University, Ethiopia.
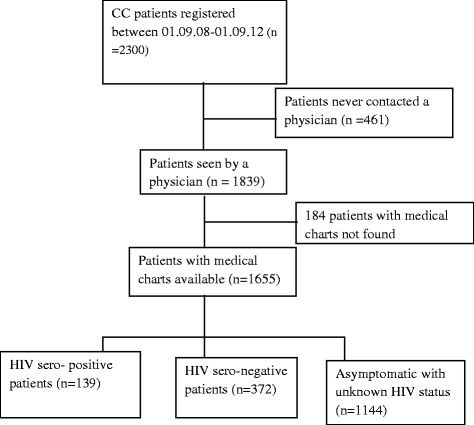
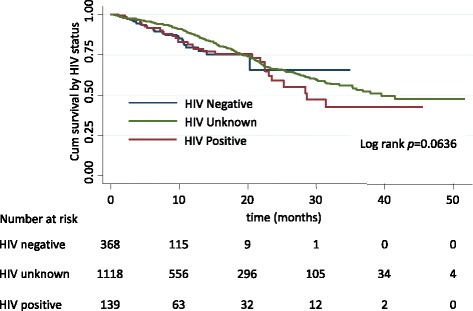
We conducted a retrospective cohort study. Data from 1655 CCPs diagnosed between September 2008 and September 2012 were included. The primary endpoint was death from any cause. Kaplan-Meier estimates were compared using the log-rank test. Cox proportional hazards regression model was used to identify predictors of death. Data were analyzed using STATA version IC/14.
The mean age of all patients was 49 years (SD = 11.6 years). Of all CCPs, 139 (8.4%) were HIV positive, 372 (22.5%) patients had a known negative HIV status and 1144 (69.1%) patients were asymptomatic with unknown HIV status. Due to late stage and waiting times, only 13.5% of the patients received curative radiotherapy doses. HIV-positive CCPs presented more often with advanced disease compared to HIV negative CCPs ((44.6%) versus 39.7%, = 0.007). There was no significant difference in survival between HIV-positive and HIV-negative CCPs. Older age (HR = 2.01; 95% CI, 1.01,-4.05), advanced disease (HR = 2.6; 95% CI, 1.67-4.04) and baseline anemia (HR = 1.65; 95% CI, 1.24, 2.20) were independent predictors for higher risk of death.
Survival rates of CCPs did not differ according to HIV status. The risk of death was higher for patients with older age, advanced disease and anemia. HIV patients should be screened for CC according to guidelines to avoid late presentation.
感染人类免疫缺陷病毒(HIV)的女性被认为患宫颈癌(CC)的风险更高。这是由于癌前病变向浸润性病变进展迅速。然而,有证据表明,由于抗逆转录病毒疗法(ART)和护理服务的可获得性,预计感染HIV的CC患者(CCP)的生存率和治疗结果会有所改善。
本研究的目的是调查在埃塞俄比亚亚的斯亚贝巴大学提库尔·安贝萨专科医院(TASH)放疗中心登记的CCP的临床特征和生存率。
我们进行了一项回顾性队列研究。纳入了2008年9月至2012年9月期间诊断的1655例CCP的数据。主要终点是任何原因导致的死亡。使用对数秩检验比较Kaplan-Meier估计值。使用Cox比例风险回归模型确定死亡的预测因素。使用STATA版本IC/14进行数据分析。
所有患者的平均年龄为49岁(标准差=11.6岁)。在所有CCP中,139例(8.4%)为HIV阳性,372例(22.5%)患者已知HIV状态为阴性,1144例(69.1%)患者无症状且HIV状态未知。由于疾病分期较晚和等待时间,只有13.5%的患者接受了根治性放疗剂量。与HIV阴性的CCP相比,HIV阳性的CCP更常表现为晚期疾病(分别为44.6%和39.7%,P=0.007)。HIV阳性和HIV阴性的CCP在生存率上没有显著差异。年龄较大(风险比[HR]=2.01;95%置信区间[CI],1.01-4.05)、疾病晚期(HR=2.6;95%CI,1.67-4.04)和基线贫血(HR=1.65;95%CI,1.24,2.20)是死亡风险较高的独立预测因素。
CCP的生存率不因HIV状态而异。年龄较大、疾病晚期和贫血的患者死亡风险较高。应根据指南对HIV患者进行CC筛查,以避免疾病晚期就诊。