Cuzin Lise, Pugliese Pascal, Allavena Clotilde, Rey David, Chirouze Catherine, Bani-Sadr Firouzé, Cabié André, Huleux Thomas, Poizot-Martin Isabelle, Cotte Laurent, Isnard Bagnis Corinne, Flandre Philippe
INSERM, UMR 1027, Toulouse, France; Université de Toulouse III, Toulouse, France; CHU Toulouse, COREVIH Toulouse, France.
Department of Infectious Diseases CHU Archet, Nice, France.
PLoS One. 2017 Dec 7;12(12):e0187517. doi: 10.1371/journal.pone.0187517. eCollection 2017.
We investigated whether patients receiving selected antiretroviral combinations had a higher risk of chronic kidney disease (CKD) using traditional regression modeling and a causal approach in a large prospective cohort.
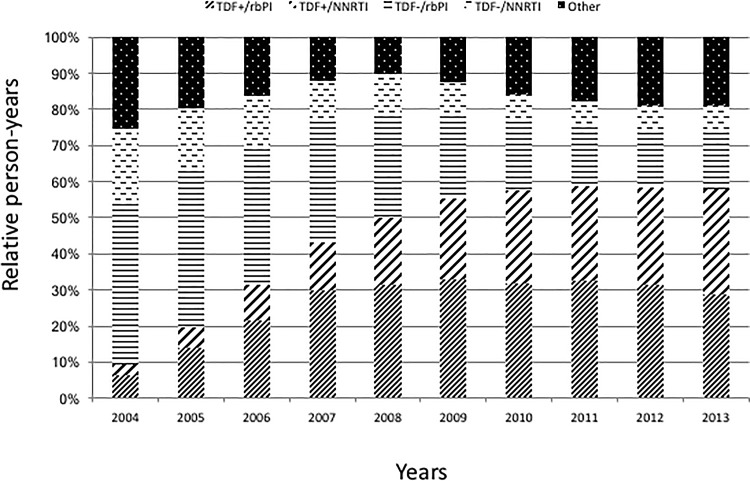
For the purpose of this study, we selected 6301 patients who (i) started their first antiretroviral regimen after 1st January 2004, (ii) had at least one serum creatinine measurement within 6 months before ART initiation (study entry), and (iii) had at least two measurements after study entry. Baseline eGFR was defined from the last serum creatinine measurement before study entry. All eGFR values were calculated using the Modification of Diet and Renal Disease (MDRD) equation. Both traditional Cox proportional hazards model and Cox marginal structural models were applied. Distinct coding for antiretroviral therapy exposure were investigated as well as double robust estimators.
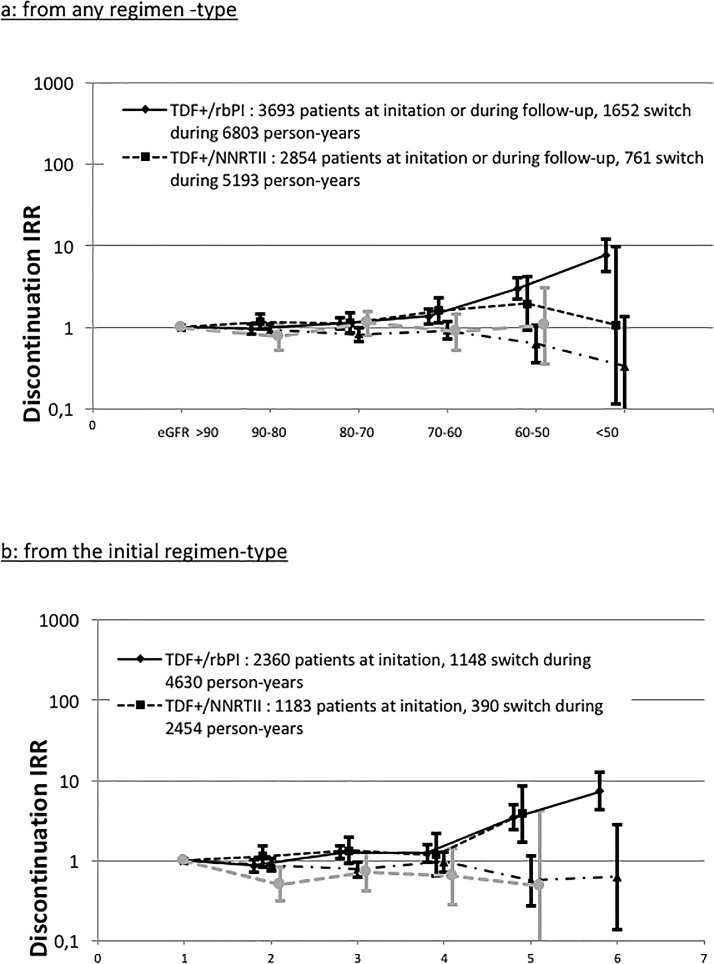
Overall we showed that patients receiving tenofovir (TDF) with a ritonavir boosted protease inhibitor (rbPI) exhibited a higher risk of CKD compared with patients who received TDF with a non-nucleosidic reverse transcriptase inhibitor (NNRTI). Such an increased risk was observed considering both initial and current regimens. Our analysis revealed a clinician-driven switch away from TDF among persons experiencing a decline in renal function while receiving this drug.
Our results show that combination of TDF and boosted protease inhibitor is associated with a higher CKD risk than TDF and a NNRTI.
我们在一个大型前瞻性队列中,使用传统回归模型和因果分析方法,研究接受特定抗逆转录病毒药物组合治疗的患者患慢性肾脏病(CKD)的风险是否更高。
在本研究中,我们选取了6301例患者,这些患者(i)在2004年1月1日之后开始其首个抗逆转录病毒治疗方案,(ii)在开始抗逆转录病毒治疗(研究入组)前6个月内至少有一次血清肌酐测量值,并且(iii)在研究入组后至少有两次测量值。基线估算肾小球滤过率(eGFR)根据研究入组前最后一次血清肌酐测量值确定。所有eGFR值均使用饮食与肾脏疾病改良(MDRD)方程计算。同时应用了传统的Cox比例风险模型和Cox边际结构模型。研究了抗逆转录病毒治疗暴露的不同编码以及双重稳健估计量。
总体而言,我们发现接受替诺福韦(TDF)与利托那韦增强型蛋白酶抑制剂(rbPI)联合治疗的患者,与接受TDF与非核苷类逆转录酶抑制剂(NNRTI)联合治疗的患者相比,患CKD的风险更高。考虑初始治疗方案和当前治疗方案时均观察到这种风险增加。我们的分析显示,在接受该药物治疗时肾功能下降的患者中,临床医生会促使其停用TDF。
我们的结果表明,与TDF和NNRTI联合治疗相比,TDF与增强型蛋白酶抑制剂联合治疗与更高的CKD风险相关。