Department of Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Department of Surgery, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea.
Cancer Res Treat. 2018 Oct;50(4):1149-1163. doi: 10.4143/crt.2017.194. Epub 2017 Dec 7.
Debates exist regarding the effectiveness of adjuvant chemotherapy for stage II colon cancer. This study aimed to investigate the current status of adjuvant chemotherapy and its impact on survival for Korean stage II colon cancer patients by analyzing the National Quality Assessment data.
A total of 7,880 patientswho underwent curative resection for stage II colon adenocarcinoma between January 2011 andDecember 2014 in Koreawere selected randomly as evaluation subjects for the quality assessment. The factors that influenced overall survival were identified. The high-risk group was defined as having at least one of the following: perforation/ obstruction, lymph node harvest less than 12, lymphovascular/perineural invasion, positive resection margin, poor differentiation, or pathologic T4 stage.
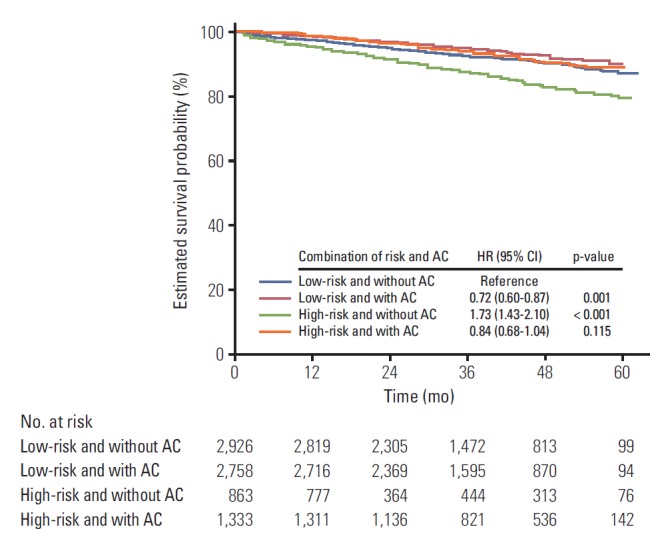
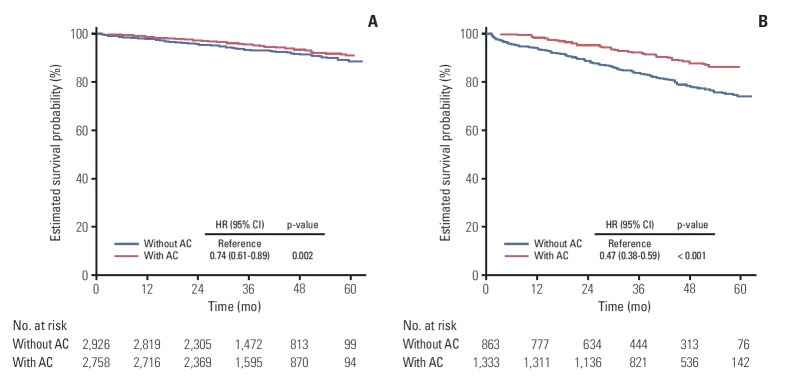
The median follow-up period was 38 months (range, 1 to 63 months). Chemotherapy was a favorable prognostic factor for either the high- (hazard ratio [HR], 0.76; 95% confidence interval [CI], 0.38 to 0.59; p < 0.001) or low-risk group (HR, 0.74; 95% CI, 0.61 to 0.89; p=0.002) in multivariate analysis. This was also the case in patients over 70 years of age. The hazard ratio was significantly increased as the number of involved risk factors was increased in patients who didn't receive chemotherapy. Adding oxaliplatin showed no difference in survival (HR, 1.36; 95% CI, 0.91 to 2.03; p=0.132).
Adjuvant chemotherapy can be recommended for stage II colon cancer patients, but the addition of oxaliplatin to the regimen must be selective.
关于 II 期结肠癌辅助化疗的疗效存在争议。本研究旨在通过分析国家质量评估数据,调查韩国 II 期结肠癌患者辅助化疗的现状及其对生存的影响。
随机选择 2011 年 1 月至 2014 年 12 月期间在韩国接受 II 期结肠癌根治性切除术的 7880 例患者作为质量评估的评价对象。确定影响总生存的因素。高危组定义为至少有以下一项:穿孔/梗阻、淋巴结采集少于 12 个、淋巴管/神经周围侵犯、阳性切缘、低分化或病理 T4 期。
中位随访时间为 38 个月(范围 1 至 63 个月)。化疗是高危组(风险比[HR],0.76;95%置信区间[CI],0.38 至 0.59;p <0.001)和低危组(HR,0.74;95% CI,0.61 至 0.89;p=0.002)多变量分析的有利预后因素。对于 70 岁以上的患者也是如此。在未接受化疗的患者中,随着受累风险因素数量的增加,风险比显著增加。添加奥沙利铂在生存方面没有差异(HR,1.36;95% CI,0.91 至 2.03;p=0.132)。
建议对 II 期结肠癌患者进行辅助化疗,但必须选择性地添加奥沙利铂方案。