Ackermann Ronald T, Wallia Amisha, O'Brien Matthew J, Kang Raymond, Cooper Andrew, Moran Margaret R, Liss David T
Department of Medicine, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA.
Institute for Public Health and Medicine, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA.
BMJ Open Diabetes Res Care. 2017 Sep 1;5(1):e000421. doi: 10.1136/bmjdrc-2017-000421. eCollection 2017.
Past research provides insufficient evidence to inform second-line diabetes medication prescribing when metformin is no longer sufficient. We evaluated patient, prescriber, and health plan characteristics associated with selection of second-line diabetes medications in the USA.
We used a multiple case-comparison study design to identify characteristics associated with the probability of starting each of six second-line diabetes medication alternatives within 77 744 adults enrolled in commercial or Medicare Advantage health plans from 2011 to 2015. National administrative data were provided by a large commercial health payer. Multinomial logistic regression models were used to identify characteristics independently associated with selecting each diabetes drug class.
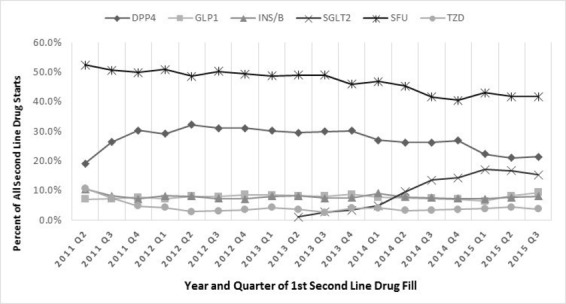
From 2011 to 2015, sulfonylureas still represented 47% of all second-line drug starts, with proportionately higher use in patients ≥75 years of age (63% of drug starts). Basal insulin was more likely to be selected when a past A1c test result was >10% (13.0% vs 4.5% for those with A1c <8%; p<0.001). Initiation of a glucagon-like peptide-1 receptor agonist was associated with being female (10.1% vs 6.0% for male; p<0.001) and having a diagnosis code for obesity (10.8% vs 6.9% for no diagnosis; p<0.001). For all drug classes, the recent prescribing behavior of the provider was a strong correlate of subsequent second-line drug selection.
Sulfonylureas continue to represent almost half of second-line diabetes medication starts in the USA. This could reflect overuse for some groups such as older adults, for whom some alternatives may be safer, although more costly and potentially less effective. Future research should compare outcomes of medication choices and conditions under which particular classes are most effective.
过去的研究提供的证据不足,无法为二甲双胍不再有效的情况下二线糖尿病药物的处方提供指导。我们评估了美国与二线糖尿病药物选择相关的患者、处方医生和健康计划特征。
我们采用多病例对照研究设计,以确定2011年至2015年参加商业或医疗保险优势健康计划的77744名成年人中开始使用六种二线糖尿病药物替代方案中每种药物的概率相关的特征。国家行政数据由一家大型商业健康支付方提供。使用多项逻辑回归模型来确定与选择每种糖尿病药物类别独立相关的特征。
2011年至2015年,磺脲类药物仍占所有二线药物起始使用的47%,在75岁及以上患者中的使用比例更高(占药物起始使用的63%)。当过去的糖化血红蛋白(A1c)检测结果>10%时,更有可能选择基础胰岛素(A1c<8%的患者为4.5%,A1c>10%的患者为13.0%;p<0.001)。启动胰高血糖素样肽-1受体激动剂与女性(女性为10.1%,男性为6.0%;p<0.001)以及有肥胖诊断代码相关(无诊断的患者为6.9%,有诊断的患者为10.8%;p<0.001)。对于所有药物类别,医生近期的处方行为与后续二线药物选择密切相关。
在美国,磺脲类药物继续占二线糖尿病药物起始使用的近一半。这可能反映了某些群体(如老年人)的过度使用,对他们来说,一些替代药物可能更安全,尽管成本更高且可能效果较差。未来的研究应比较药物选择的结果以及特定类别药物最有效的条件。