Lee Dong Hyun, Han Jinu, Han Sueng-Han, Lee Sung Chul, Kim Min
Institute of Vision Research, Department of Ophthalmology, Severance Eye and ENT Hospital, Yonsei University College of Medicine, Seoul, South Korea.
Department of Ophthalmology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, South Korea.
BMC Ophthalmol. 2017 Dec 13;17(1):249. doi: 10.1186/s12886-017-0649-2.
The authors report a case of a rare complication that occurred after botulinum toxin injection to the extraocular muscle, which was easily overlooked and successfully corrected by surgery.
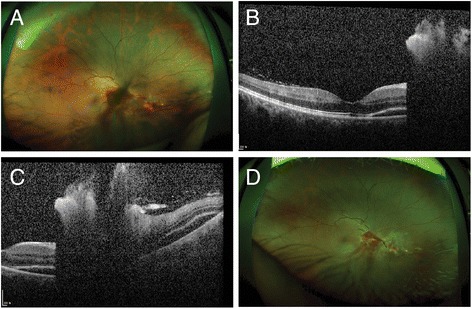
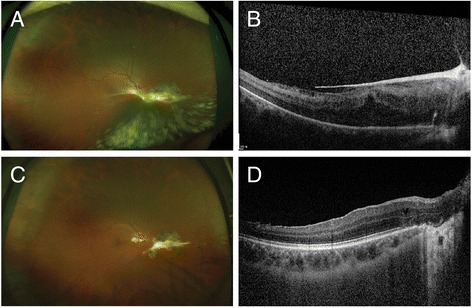
A 34-year-old female patient visited our clinic for diplopia and ocular motility disorder after removal of an epidermoid tumor of the brain. At her initial visit, her best-corrected visual acuity (BCVA) was 20/20 for both eyes. An alternate cover test showed 45 prism-diopter esotropia and 3 prism-diopter hypertropia in the right eye. Following 6 months of observation, the deviation of the strabismus did not improve, and botulinum toxin was injected into the right medial rectus (RMR). After 6 days, she visited our clinic with decreased visual acuity of her right eye. The BCVA was found to be 20/50 for her right eye. Funduscopic examination presented a retinal tear inferonasal to the optic disc with preretinal hemorrhage. Subretinal fluid nasal to the fovea was seen on optical coherence tomography (OCT). Barrier laser photocoagulation was done around the retinal tear; however, her visual acuity continued to decrease, and vitreous hemorrhage and subretinal fluid at the lesion did not improve. In addition, a newly developed epiretinal membrane was seen on OCT. An alternate cover test presented 30 prism-diopter right esotropia. 19 weeks after RMR botulinum toxin injection, she received pars plana vitrectomy, membranectomy, endolaser barrier photocoagulation, and intravitreal bevacizumab (Avastin®) injection. After 4 months, her visual acuity improved to 20/20, and only 4 prism-diopter of right hypertropia and 3 prism-diopter of exotropia were noted. Vitreous opacity and the epiretinal membrane were completely removed, as confirmed by funduscopic and examination.
Sudden loss of vision after injection of botulinum toxin into the extraocular muscle may suggest a serious complication, and a prompt, thorough ophthalmic examination should be performed. If improvements are not observed, rapid surgical intervention is recommended to prevent additional complications.
作者报告了1例肉毒杆菌毒素注射至眼外肌后发生的罕见并发症,该并发症易被忽视,但通过手术成功矫正。
一名34岁女性患者因脑表皮样瘤切除术后出现复视和眼球运动障碍前来我院就诊。初诊时,她双眼的最佳矫正视力(BCVA)均为20/20。交替遮盖试验显示右眼有45棱镜度的内斜视和3棱镜度的上斜视。经过6个月的观察,斜视偏差未改善,遂向右眼内直肌(RMR)注射肉毒杆菌毒素。6天后,她因右眼视力下降前来我院就诊。发现其右眼BCVA为20/50。眼底检查显示视盘鼻下象限有视网膜裂孔并伴有视网膜前出血。光学相干断层扫描(OCT)显示黄斑鼻侧有视网膜下液。在视网膜裂孔周围进行了屏障激光光凝;然而,她的视力继续下降,病变处的玻璃体积血和视网膜下液未改善。此外,OCT上可见新形成的视网膜前膜。交替遮盖试验显示右眼有30棱镜度的外斜视。在RMR注射肉毒杆菌毒素19周后,她接受了玻璃体切除术、膜切除术、眼内激光屏障光凝和玻璃体内注射贝伐单抗(阿瓦斯汀®)。4个月后,她的视力提高到20/20,仅右眼有4棱镜度的上斜视和3棱镜度的外斜视。眼底检查和检查证实玻璃体混浊和视网膜前膜已完全清除。
向眼外肌注射肉毒杆菌毒素后突然视力丧失可能提示严重并发症,应立即进行全面、彻底的眼科检查。如果未观察到改善,建议迅速进行手术干预以预防其他并发症。