Alam Shirjel R, Stirrat Colin, Spath Nick, Zamvar Vipin, Pessotto Renzo, Dweck Marc R, Moore Colin, Semple Scott, El-Medany Ahmed, Manoharan Divya, Mills Nicholas L, Shah Anoop, Mirsadraee Saeed, Newby David E, Henriksen Peter A
BHF Centre for Cardiovascular Science, University of Edinburgh, The Chancellor's Building, Little France Crescent, Edinburgh, EH16 5SA, UK.
Department of Cardiothoracic Surgery, Edinburgh Heart Centre, Edinburgh, UK.
J Cardiothorac Surg. 2017 Dec 16;12(1):115. doi: 10.1186/s13019-017-0681-6.
Myocardial inflammation and injury occur during coronary artery bypass graft (CABG) surgery. We aimed to characterise these processes during routine CABG surgery to inform the diagnosis of type 5 myocardial infarction.
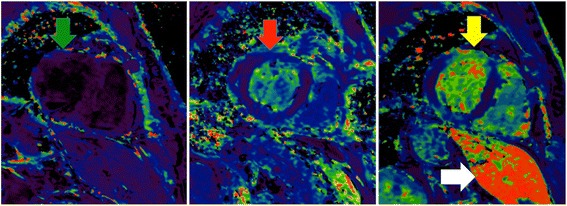
We assessed 87 patients with stable coronary artery disease who underwent elective CABG surgery. Myocardial inflammation, injury and infarction were assessed using plasma inflammatory biomarkers, high-sensitivity cardiac troponin I (hs-cTnI) and cardiac magnetic resonance imaging (CMR) using both late gadolinium enhancement (LGE) and ultrasmall superparamagnetic particles of iron oxide (USPIO).
Systemic humoral inflammatory biomarkers (myeloperoxidase, interleukin-6, interleukin-8 and c-reactive protein) increased in the post-operative period with C-reactive protein concentrations plateauing by 48 h (median area under the curve (AUC) 7530 [interquartile range (IQR) 6088 to 9027] mg/L/48 h). USPIO-defined cellular myocardial inflammation ranged from normal to those associated with type 1 myocardial infarction (median 80.2 [IQR 67.4 to 104.8] /s). Plasma hs-cTnI concentrations rose by ≥50-fold from baseline and exceeded 10-fold the upper limit of normal in all patients. Two distinct patterns of peak cTnI release were observed at 6 and 24 h. After CABG surgery, new LGE was seen in 20% (n = 18) of patients although clinical peri-operative type 5 myocardial infarction was diagnosed in only 9% (n = 8). LGE was associated with the delayed 24-h peak in hs-cTnI and its magnitude correlated with AUC plasma hs-cTnI concentrations (r = 0.33, p < 0.01) but not systemic inflammation, myocardial inflammation or bypass time.
Patients undergoing CABG surgery invariably have plasma hs-cTnI concentrations >10-fold the 99th centile upper limit of normal that is not attributable to inflammatory or ischemic injury alone. Peri-operative type 5 myocardial infarction is often unrecognised and is associated with a delayed 24-h peak in plasma hs-cTnI concentrations.
在冠状动脉旁路移植术(CABG)手术期间会发生心肌炎症和损伤。我们旨在对常规CABG手术期间的这些过程进行特征描述,以为5型心肌梗死的诊断提供依据。
我们评估了87例接受择期CABG手术的稳定型冠状动脉疾病患者。使用血浆炎症生物标志物、高敏心肌肌钙蛋白I(hs-cTnI)以及采用延迟钆增强(LGE)和超小超顺磁性氧化铁颗粒(USPIO)的心脏磁共振成像(CMR)来评估心肌炎症、损伤和梗死情况。
全身体液炎症生物标志物(髓过氧化物酶、白细胞介素-6、白细胞介素-8和C反应蛋白)在术后期间升高,C反应蛋白浓度在48小时时达到平稳(曲线下面积(AUC)中位数为7530 [四分位间距(IQR)6088至9027] mg/L/48小时)。USPIO定义的细胞性心肌炎症范围从正常到与1型心肌梗死相关的炎症(中位数为80.2 [IQR 67.4至104.8] /s)。所有患者血浆hs-cTnI浓度从基线升高≥50倍,且超过正常上限的10倍。观察到在6小时和24小时出现两种不同的cTnI释放峰值模式。CABG手术后,20%(n = 18)的患者出现了新的LGE,尽管围手术期仅9%(n = 8)的患者被诊断为临床5型心肌梗死。LGE与hs-cTnI的延迟24小时峰值相关,其程度与血浆hs-cTnI浓度的AUC相关(r = 0.33,p < 0.01),但与全身炎症、心肌炎症或旁路时间无关。
接受CABG手术的患者血浆hs-cTnI浓度总是超过正常第99百分位数上限的10倍,这并非仅由炎症或缺血性损伤所致。围手术期5型心肌梗死常常未被识别,且与血浆hs-cTnI浓度的延迟24小时峰值相关。