Harries Rhiannon L, Cornish Julie, Bosanquet David, Rees Buddug, Horwood James, Islam Saiful, Bashir Nadim, Watkins Alan, Russell Ian T, Torkington Jared
Department of Colorectal Surgery, University Hospital of Wales, Cardiff, UK.
Welsh Barbers Research Group, Cardiff, UK.
BMJ Open. 2017 Dec 19;7(12):e017235. doi: 10.1136/bmjopen-2017-017235.
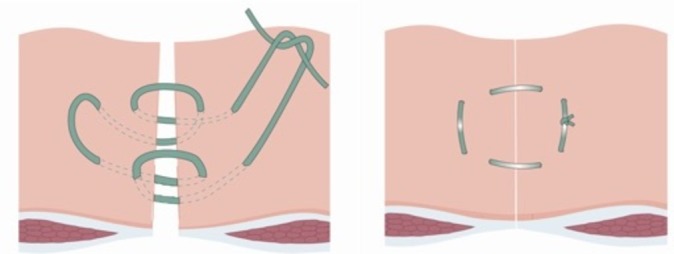
Incisional hernias are common complications of midline abdominal closure. The 'Hughes Repair' combines a standard mass closure with a series of horizontal and two vertical mattress sutures within a single suture. There is evidence to suggest this technique is as effective as mesh repair for the operative management of incisional hernias; however, no trials have compared Hughes repair with standard mass closure for the prevention of incisional hernia formation. This paper aims to test the feasibility of running a randomised controlled trial of a comparison of abdominal wall closure methods following midline incisional surgery for colorectal cancer, in preparation to a definitive randomised controlled trial.
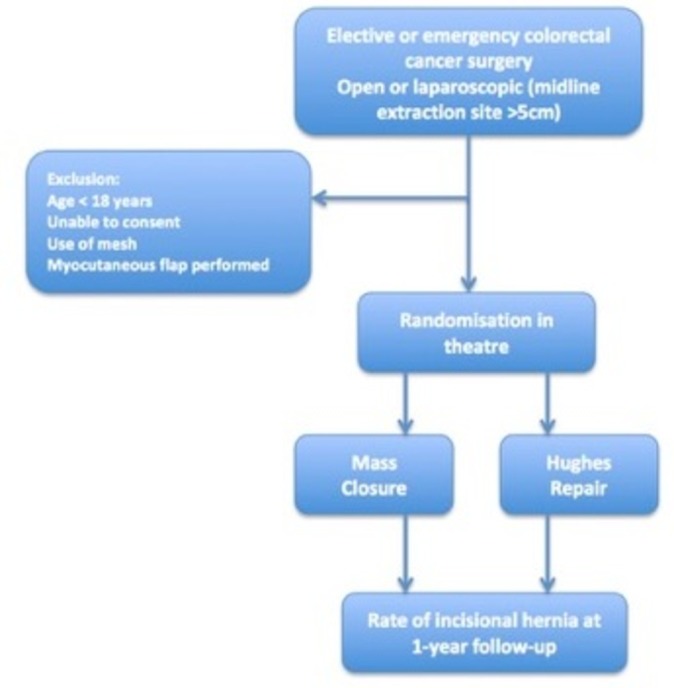
A feasibility trial (with 1:1 randomisation) conducted perioperatively during colorectal cancer surgery.
Patients undergoing midline incisional surgery for resection of colorectal cancer.
Comparison of two suture techniques (Hughes repair or standard mass closure) for the closure of the midline abdominal wound following surgery for colorectal cancer.
A 30-patient feasibility trial assessed recruitment, randomisation, deliverability and early safety of the surgical techniques used.
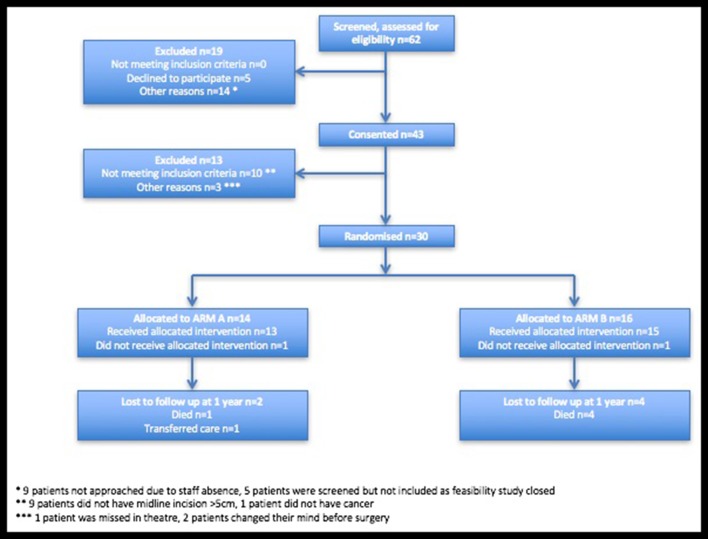
A total of 30 patients were randomised from 43 patients recruited and consented, over a 5-month period. 14 and 16 patients were randomised to arms A and B, respectively. There was one superficial surgical site infection (SSI) and two organ space SSIs reported in arm A, and two superficial SSIs and one complete wound dehiscence in arm B. There were no suspected unexpected serious adverse reactions reported in either arm. Independent data monitoring committee found no early safety concerns.
The feasibility trial found no early safety concerns and demonstrated that the trial was acceptable to patients. Progression to the pilot and main phases of the trial has now commenced following approval by the independent data monitoring committee.
ISRCTN 25616490.
切口疝是腹部正中切口关闭后的常见并发症。“休斯修补术”将标准的整块缝合与单根缝线内的一系列水平和两根垂直褥式缝线相结合。有证据表明,该技术在切口疝的手术治疗中与补片修补术同样有效;然而,尚无试验比较休斯修补术与标准整块缝合术预防切口疝形成的效果。本文旨在测试对结直肠癌中线切开手术后腹壁关闭方法进行比较的随机对照试验的可行性,为最终的随机对照试验做准备。
在结直肠癌手术围手术期进行的一项可行性试验(1:1随机分组)。
接受中线切开手术切除结直肠癌的患者。
比较两种缝合技术(休斯修补术或标准整块缝合术)在结直肠癌手术后关闭腹部正中伤口的效果。
一项纳入30例患者的可行性试验评估了所使用手术技术的招募、随机分组、可实施性和早期安全性。
在5个月的时间里,从43例招募并同意参与的患者中随机选取了30例。分别有14例和16例患者被随机分配到A组和B组。A组报告了1例浅表手术部位感染(SSI)和2例器官间隙SSI,B组报告了2例浅表SSI和1例完全伤口裂开。两组均未报告疑似意外严重不良反应。独立数据监测委员会未发现早期安全问题。
可行性试验未发现早期安全问题,并表明该试验对患者是可接受的。经独立数据监测委员会批准后,现已开始进入试验的试点和主要阶段。
ISRCTN 25616490。