Cornish J, Harries R L, Bosanquet D, Rees B, Ansell J, Frewer N, Dhruva Rao P K, Parry C, Ellis-Owen R, Phillips S M, Morris C, Horwood J, Davies M L, Davies M M, Hargest R, Davies Z, Hilton J, Harris D, Ben-Sassi A, Rajagopal R, Hanratty D, Islam S, Watkins A, Bashir N, Jones S, Russell I R, Torkington J
Department of Surgery, University Hospital of Wales, Heath Park, Cardiff, CF14 4XW, UK.
Princess of Wales Hospital, Bridgend, UK.
Trials. 2016 Sep 15;17(1):454. doi: 10.1186/s13063-016-1573-0.
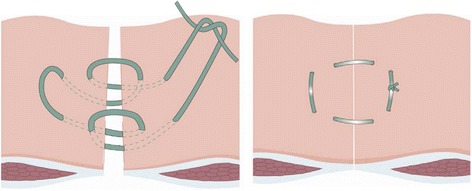
Incisional hernias are common complications of midline closure following abdominal surgery and cause significant morbidity, impaired quality of life and increased health care costs. The 'Hughes Repair' combines a standard mass closure with a series of horizontal and two vertical mattress sutures within a single suture. This theoretically distributes the load along the incision length as well as across it. There is evidence to suggest that this technique is as effective as mesh repair for the operative management of incisional hernias; however, no trials have compared the Hughes Repair with standard mass closure for the prevention of incisional hernia formation following a midline incision.
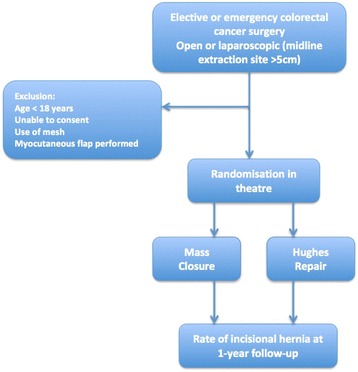
METHODS/DESIGN: This is a 1:1 randomised controlled trial comparing two suture techniques for the closure of the midline abdominal wound following surgery for colorectal cancer. Full ethical approval has been gained (Wales REC 3, MREC 12/WA/0374). Eight hundred patients will be randomised from approximately 20 general surgical units within the United Kingdom. Patients undergoing open or laparoscopic (more than a 5-cm midline incision) surgery for colorectal cancer, elective or emergency, are eligible. Patients under the age of 18 years, those having mesh inserted or undergoing musculofascial flap closure of the perineal defect in abdominoperineal wound closure, and those unable to give informed consent will be excluded. Patients will be randomised intraoperatively to either the Hughes Repair or standard mass closure. The primary outcome measure is the incidence of incisional hernias at 1 year as assessed by standardised clinical examination. The secondary outcomes include quality of life patient-reported outcome measures, cost-utility analysis, incidence of complete abdominal wound dehiscence and C-POSSUM scores. The incidence of incisional hernia at 1 year, assessed by computerised tomography, will form a tertiary outcome.
A feasibility phase has been completed. The results of the study will be used to inform current and future practice and potentially reduce the risk of incisional hernia formation following midline incisions.
ISRCTN 25616490 . Registered on 1 January 2012.
切口疝是腹部手术后中线缝合常见的并发症,会导致严重的发病率、生活质量受损以及医疗费用增加。“休斯修补术”将标准的整块缝合与一系列水平和两条垂直褥式缝合结合在一根缝线内。从理论上讲,这能将负荷沿切口长度以及切口宽度进行分布。有证据表明,该技术在切口疝的手术治疗中与补片修补术效果相当;然而,尚无试验将休斯修补术与标准整块缝合用于预防中线切口后切口疝形成进行比较。
方法/设计:这是一项1:1随机对照试验,比较两种缝合技术用于结直肠癌手术后腹部中线伤口的缝合。已获得全面伦理批准(威尔士研究伦理委员会3号,医学研究伦理委员会12/WA/0374)。将从英国约20个普通外科病房随机选取800例患者。接受开放性或腹腔镜(中线切口超过5厘米)手术的结直肠癌患者,无论是择期还是急诊手术,均符合条件。18岁以下患者、在腹会阴伤口缝合中植入补片或进行会阴缺损肌筋膜瓣闭合的患者以及无法给予知情同意的患者将被排除。患者将在术中随机分为休斯修补术组或标准整块缝合组。主要结局指标是术后一年通过标准化临床检查评估的切口疝发生率。次要结局包括患者报告的生活质量结局指标、成本效用分析、腹部伤口完全裂开的发生率以及C-POSSUM评分。通过计算机断层扫描评估的术后一年切口疝发生率将作为三级结局。
可行性阶段已完成。该研究结果将用于指导当前和未来的实践,并有可能降低中线切口后切口疝形成的风险。
ISRCTN 25616490。于2012年1月1日注册。