Pineda Silvia, Sigdel Tara K, Chen Jieming, Jackson Annette M, Sirota Marina, Sarwal Minnie M
Division of Transplant Surgery, Department of Surgery, University of California, San Francisco (UCSF), San Francisco, CA, United States.
Institute for Computational Health Sciences, University of California, San Francisco (UCSF), San Francisco, CA, United States.
Front Immunol. 2017 Dec 5;8:1687. doi: 10.3389/fimmu.2017.01687. eCollection 2017.
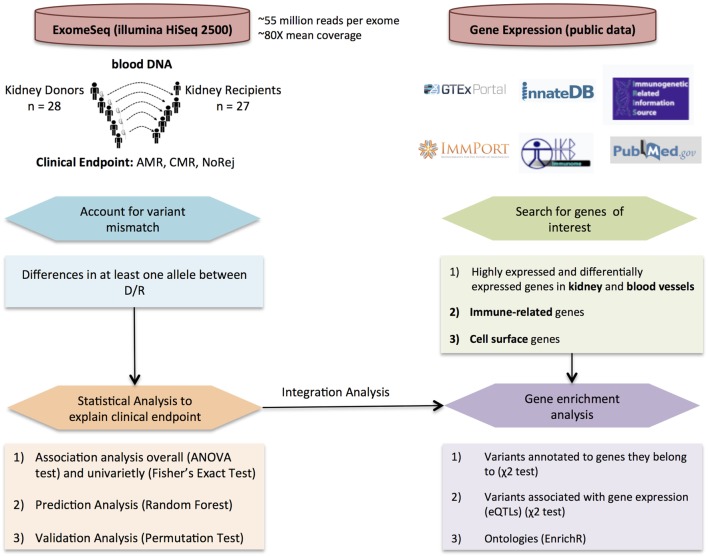
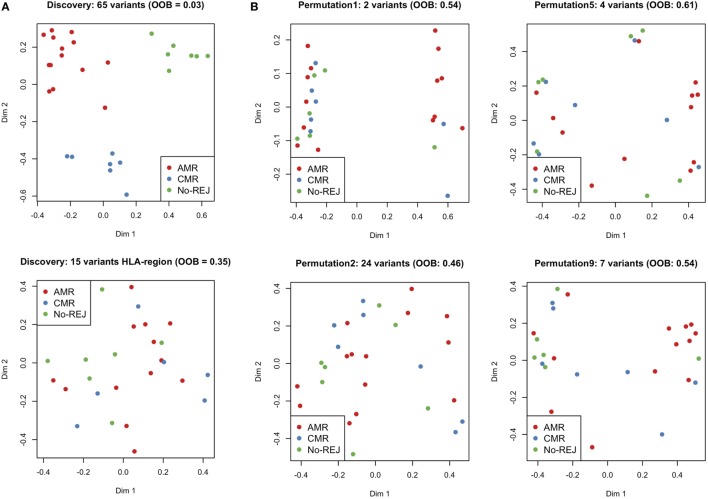
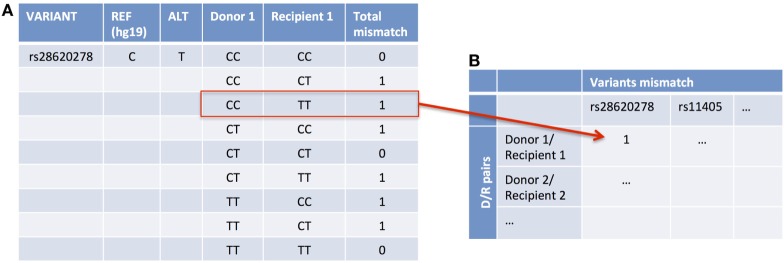
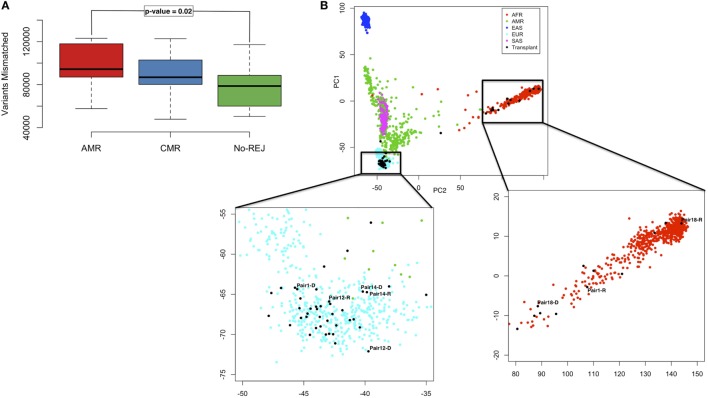
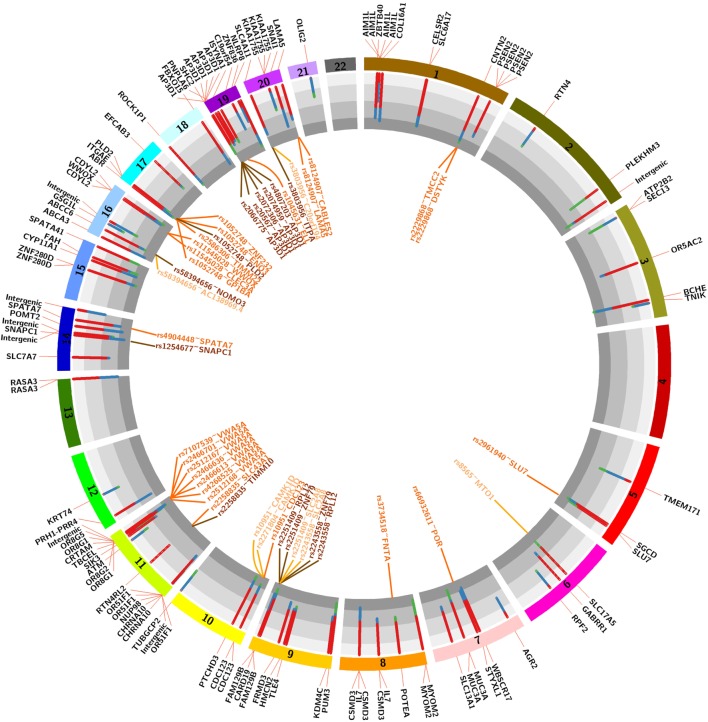
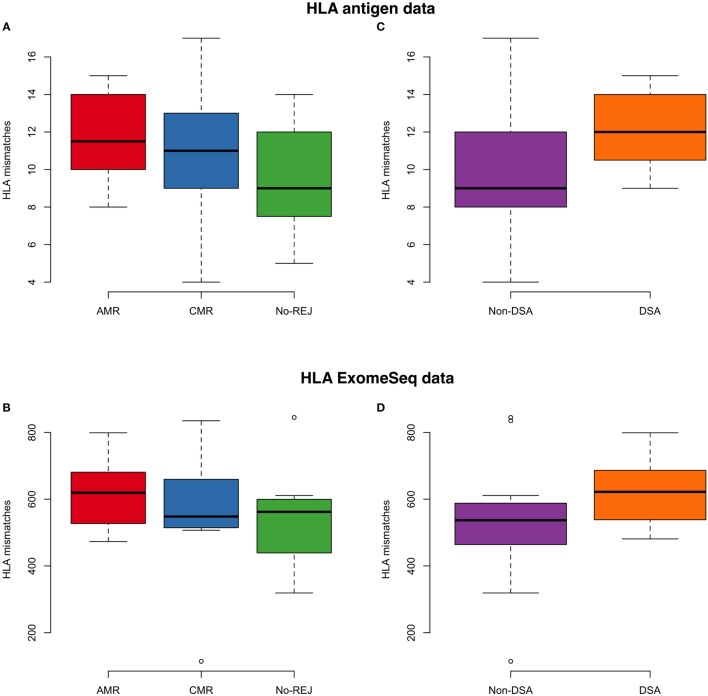
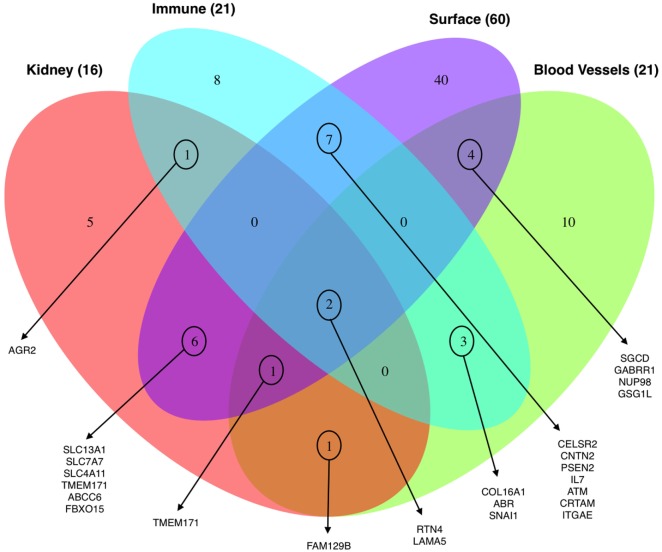
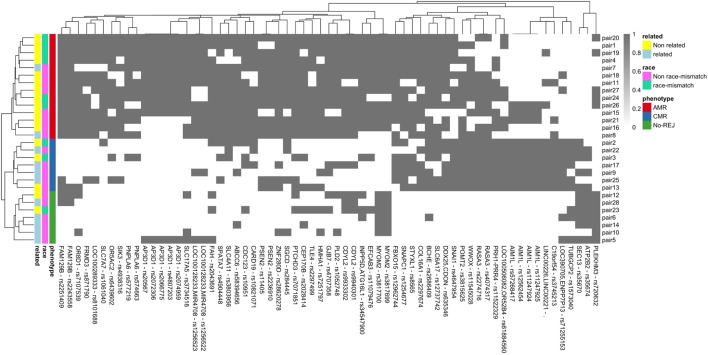
Transplant rejection is the critical clinical end-point limiting indefinite survival after histocompatibility antigen (HLA) mismatched organ transplantation. The predominant cause of late graft loss is antibody-mediated rejection (AMR), a process whereby injury to the organ is caused by donor-specific antibodies, which bind to HLA and non-HLA (nHLA) antigens. AMR is incompletely diagnosed as donor/recipient (D/R) matching is only limited to the HLA locus and critical nHLA immunogenic antigens remain to be identified. We have developed an integrative computational approach leveraging D/R exome sequencing and gene expression to predict clinical post-transplant outcome. We performed a rigorous statistical analysis of 28 highly annotated D/R kidney transplant pairs with biopsy-confirmed clinical outcomes of rejection [either AMR or T-cell-mediated rejection (CMR)] and no-rejection (NoRej), identifying a significantly higher number of mismatched nHLA variants in AMR (ANOVA--value = 0.02). Using Fisher's exact test, we identified 123 variants associated mainly with risk of AMR (-value < 0.001). In addition, we applied a machine-learning technique to circumvent the issue of statistical power and we found a subset of 65 variants using random forest, that are predictive of post-tx AMR showing a very low error rate. These variants are functionally relevant to the rejection process in the kidney and AMR as they relate to genes and/or expression quantitative trait loci (eQTLs) that are enriched in genes expressed in kidney and vascular endothelium and underlie the immunobiology of graft rejection. In addition to current D/R HLA mismatch evaluation, additional mismatch nHLA D/R variants will enhance the stratification of post-tx AMR risk even before engraftment of the organ. This innovative study design is applicable in all solid organ transplants, where the impact of mitigating AMR on graft survival may be greater, with considerable benefits on improving human morbidity and mortality and opens the door to precision immunosuppression and extended tx survival.
移植排斥是限制组织相容性抗原(HLA)不匹配器官移植后长期存活的关键临床终点。晚期移植物丢失的主要原因是抗体介导的排斥反应(AMR),这一过程中,供体特异性抗体与HLA和非HLA(nHLA)抗原结合,导致器官损伤。由于供体/受体(D/R)匹配仅局限于HLA位点,且关键的nHLA免疫原性抗原仍有待确定,AMR的诊断并不完全。我们开发了一种综合计算方法,利用D/R外显子组测序和基因表达来预测移植后的临床结果。我们对28对经过严格注释的D/R肾移植配对进行了严谨的统计分析,这些配对具有活检确诊的排斥反应(AMR或T细胞介导的排斥反应(CMR))和无排斥反应(NoRej)的临床结果,发现AMR中不匹配的nHLA变体数量显著更多(方差分析——P值 = 0.02)。使用Fisher精确检验,我们鉴定出123个主要与AMR风险相关的变体(P值 < 0.001)。此外,我们应用机器学习技术来解决统计效力问题,通过随机森林发现了一个由65个变体组成的子集,这些变体可预测移植后AMR,显示出非常低的错误率。这些变体在功能上与肾脏和AMR的排斥过程相关,因为它们与在肾脏和血管内皮中表达的基因以及构成移植排斥免疫生物学基础的基因和/或表达数量性状位点(eQTL)相关。除了当前的D/R HLA错配评估外,额外的不匹配nHLA D/R变体将在器官植入前增强对移植后AMR风险的分层。这种创新的研究设计适用于所有实体器官移植,在这些移植中减轻AMR对移植物存活的影响可能更大,对改善人类发病率和死亡率有相当大的益处,并为精准免疫抑制和延长移植存活期打开了大门。