Sato Yuki, Yanagita Motoko
Medical Innovation Center, TMK project, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
Department of Nephrology, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
Inflamm Regen. 2017 Aug 7;37:17. doi: 10.1186/s41232-017-0048-3. eCollection 2017.
Chronic kidney disease (CKD) is a leading cause of end stage renal disease (ESRD) and cardiovascular morbidity and mortality worldwide, resulting in a growing social and economic burden. The prevalence and burden of CKD is anticipated to further increase over the next decades as a result of aging.
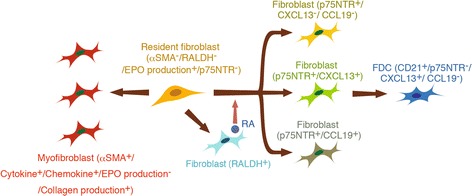
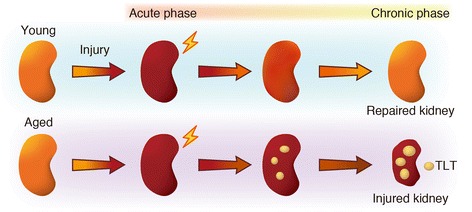
In the pathogenesis of CKD, irrespective of the etiology, resident fibroblasts are key players and have been demonstrated to play crucial roles for disease initiation and progression. In response to injury, resident fibroblasts transdifferentiate into myofibroblasts that express alpha smooth muscle actin (αSMA) and have an increased capacity to produce large amounts of extracellular matrix (ECM) proteins, leading to renal fibrosis. In addition to this fundamental role of fibroblasts as drivers for renal fibrosis, growing amounts of evidence have shown that resident fibroblasts are also actively involved in initiating and promoting inflammation during kidney injury. During the myofibroblastic transition described above, resident fibroblasts activate NF-κB signaling and produce pro-inflammatory cytokines and chemokines, promoting inflammation. Furthermore, under aging milieu, resident fibroblasts transdifferentiate into several distinct phenotypic fibroblasts, including CXCL13/CCL19-producing fibroblasts, retinoic acid-producing fibroblasts, and follicular dendritic cells, in response to injury and orchestrate tertiary lymphoid tissue (TLT) formation, which results in uncontrolled aberrant inflammation and retards tissue repair. Anti-inflammatory agents can improve myofibroblastic transdifferentiation and abolish TLT formation, suggesting that targeting these inflammatory fibroblasts can potentially ameliorate kidney disease.
Beyond its conventional role as an executor of fibrosis, resident fibroblasts display more pro-inflammatory phenotypes and contribute actively to driving inflammation during kidney injury.
慢性肾脏病(CKD)是全球终末期肾病(ESRD)以及心血管疾病发病和死亡的主要原因,导致社会和经济负担日益加重。由于老龄化,预计在未来几十年中CKD的患病率和负担将进一步增加。
在CKD的发病机制中,无论病因如何,肾脏驻留成纤维细胞都是关键参与者,并且已被证明在疾病的发生和发展中起关键作用。在受到损伤时,肾脏驻留成纤维细胞转分化为肌成纤维细胞,这些肌成纤维细胞表达α平滑肌肌动蛋白(αSMA),并具有更强的能力来产生大量细胞外基质(ECM)蛋白,从而导致肾纤维化。除了成纤维细胞作为肾纤维化驱动因素的这一基本作用外,越来越多的证据表明,肾脏驻留成纤维细胞在肾脏损伤期间也积极参与启动和促进炎症反应。在上述肌成纤维细胞转变过程中,肾脏驻留成纤维细胞激活核因子κB信号通路并产生促炎细胞因子和趋化因子,从而促进炎症反应。此外,在衰老环境下,肾脏驻留成纤维细胞在受到损伤时会转分化为几种不同表型的成纤维细胞,包括产生CXCL13/CCL19的成纤维细胞、产生视黄酸的成纤维细胞和滤泡树突状细胞,并协调三级淋巴组织(TLT)的形成,这会导致不受控制的异常炎症反应并阻碍组织修复。抗炎药物可以改善肌成纤维细胞转分化并消除TLT的形成,这表明靶向这些炎症性成纤维细胞可能会改善肾脏疾病。
除了作为纤维化执行者的传统作用外,肾脏驻留成纤维细胞还表现出更多的促炎表型,并在肾脏损伤期间积极促进炎症反应。