Hanley James A, Hannigan Ailish, O'Brien Katie M
Department of Epidemiology, Biostatistics, and Occupational Health, McGill University, Montréal, Québec, Canada.
Graduate Entry Medical School, University of Limerick, Limerick, Ireland.
PLoS One. 2017 Dec 20;12(12):e0188947. doi: 10.1371/journal.pone.0188947. eCollection 2017.
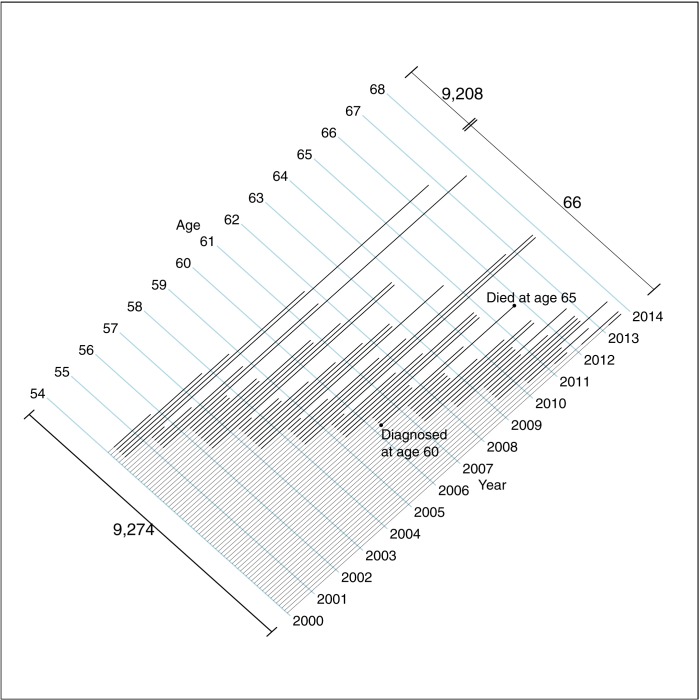
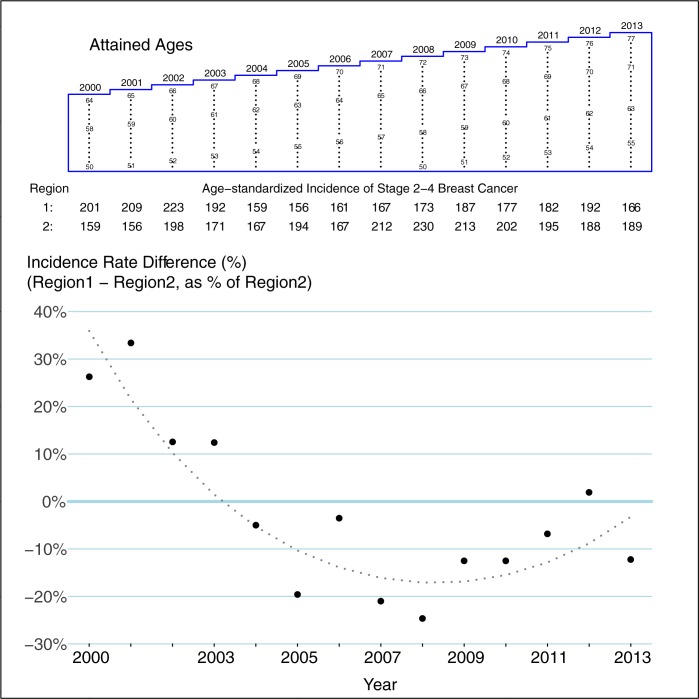
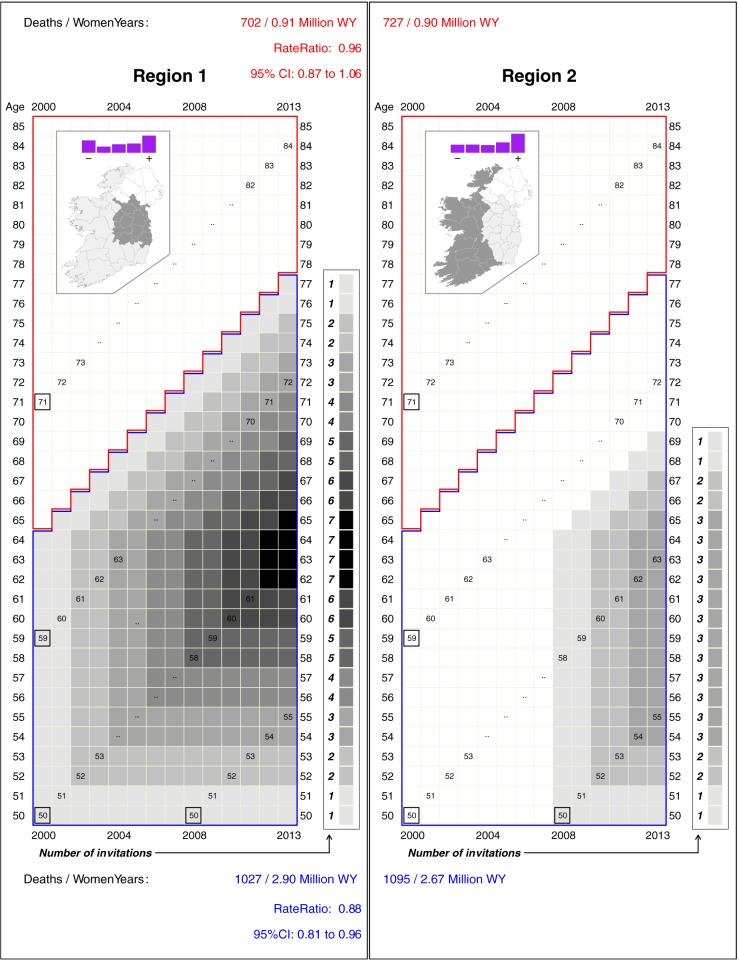
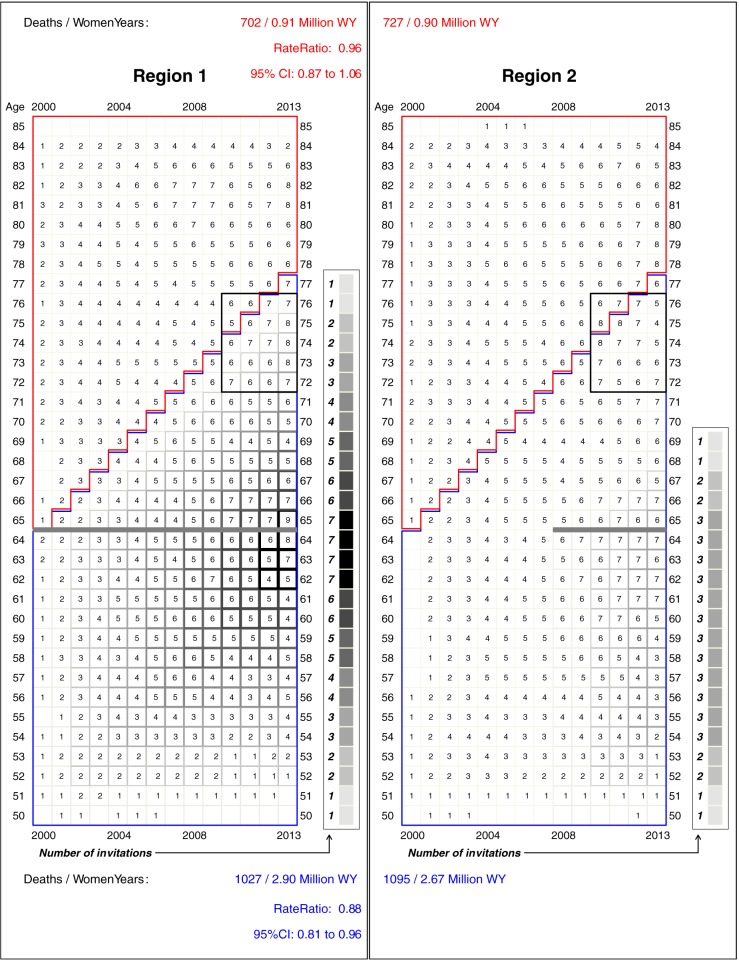
Our objective was to compare breast cancer mortality in two regions of the Republic of Ireland that introduced a screening programme eight years apart, and to estimate the steady-state mortality deficits the programme will produce. We carried out age- and year-matched between-region comparison of breast cancer mortality rates, and of incidence rates of stage 2-4 breast cancer, in the eligible cohorts. The regions comprised counties that, beginning in early 2000 (region 1) and late 2007 (region 2), invited women aged 50-64 to biennial mammography screening. The data were supplied by the National Cancer Registry, Central Statistics Office. As impact measures, we used age-and-year-matched mortality (from breast cancers diagnosed from 2000 onwards), rate ratios and incidence rate ratios in the compared regions from 2000 to 2013. Ratios were adjusted for between-region differences in background rates. In cohorts too old to be invited, death rates in regions 1 and 2 were 702 per 0.91 and 727 per 0.90 million women-years respectively (Ratio 0.96). In the eligible cohorts, they were 1027 per 2.9 and 1095 per 2.67 (Ratio 0.88). Thus, rates in cohorts that could have benefitted were 9% lower in region 1 than region 2: (95%CI: -20%, +4%). The incidence rates of stage 2-4 breast cancer were 7% lower in region 2 than region 1 over the entire 14 year period, and 20% lower in 2007, i.e., before the screening in region 2 began to narrow the difference. Since mortality reductions due to screening only manifest after several years, the full impact of screening has not yet been realized in region 1. The lower rate observed in that region is a conservative estimate of the steady state benefit. Additional deaths would have been averted had screening continued beyond age 64.
我们的目标是比较爱尔兰共和国两个地区的乳腺癌死亡率,这两个地区相隔八年引入了筛查计划,并估计该计划将产生的稳态死亡率降低幅度。我们对符合条件的队列进行了年龄和年份匹配的地区间乳腺癌死亡率以及2 - 4期乳腺癌发病率的比较。这两个地区包括一些县,从2000年初(地区1)和2007年末(地区2)开始,邀请50 - 64岁的女性进行两年一次的乳房X光筛查。数据由中央统计局国家癌症登记处提供。作为影响指标,我们使用了年龄和年份匹配的死亡率(来自2000年及以后诊断出的乳腺癌)、2000年至2013年比较地区的率比和发病率比。率比针对地区间背景率差异进行了调整。在年龄太大而未被邀请的队列中,地区1和地区2的死亡率分别为每0.91百万女性年702例和每0.90百万女性年727例(比率0.96)。在符合条件的队列中,分别为每2.9百万女性年1027例和每2.67百万女性年1095例(比率0.88)。因此,可能受益的队列中,地区1的死亡率比地区2低9%:(95%置信区间:-20%,+4%)。在整个14年期间,地区2的2 - 4期乳腺癌发病率比地区1低7%,在2007年低20%,即在地区2筛查开始缩小差异之前。由于筛查导致的死亡率降低要在几年后才会显现,地区1尚未实现筛查的全部影响。该地区观察到的较低比率是稳态益处的保守估计。如果筛查年龄超过64岁,本可避免更多死亡。