Mallappa Ashwini, Nella Aikaterini A, Kumar Parag, Brooks Kristina M, Perritt Ashley F, Ling Alexander, Liu Chia-Ying, Merke Deborah P
National Institutes of Health Clinical Center, Bethesda, Maryland 20892.
Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, Maryland 20892.
J Endocr Soc. 2017 Jun 21;1(7):994-1001. doi: 10.1210/js.2017-00215. eCollection 2017 Jul 1.
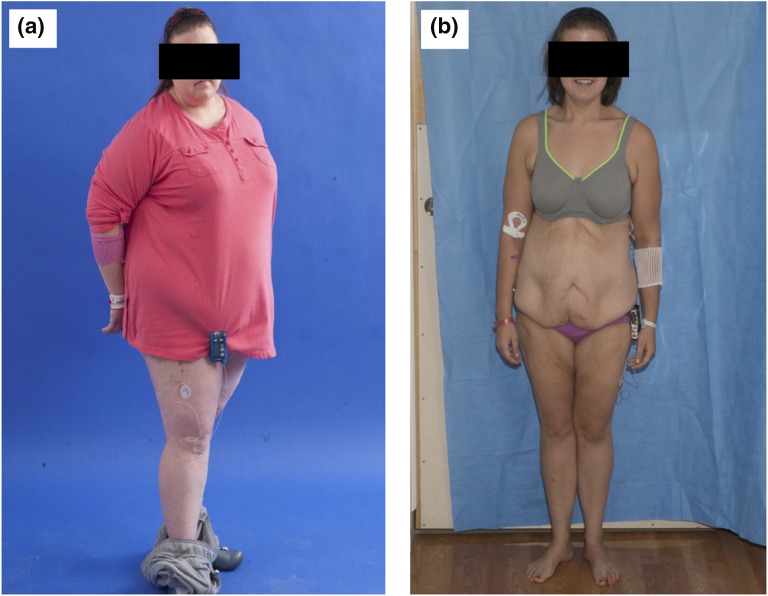
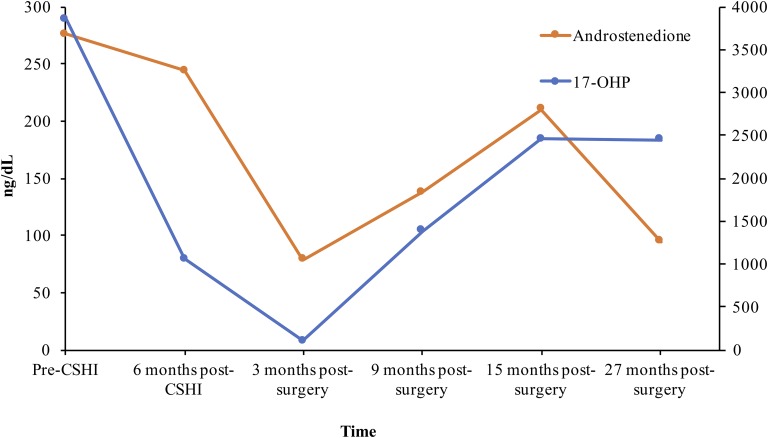
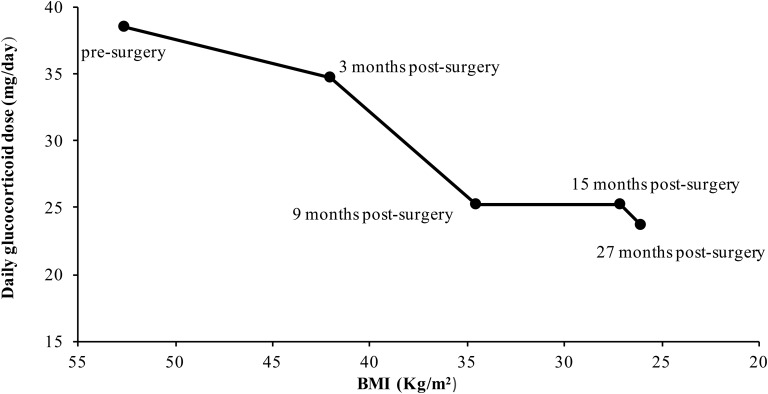
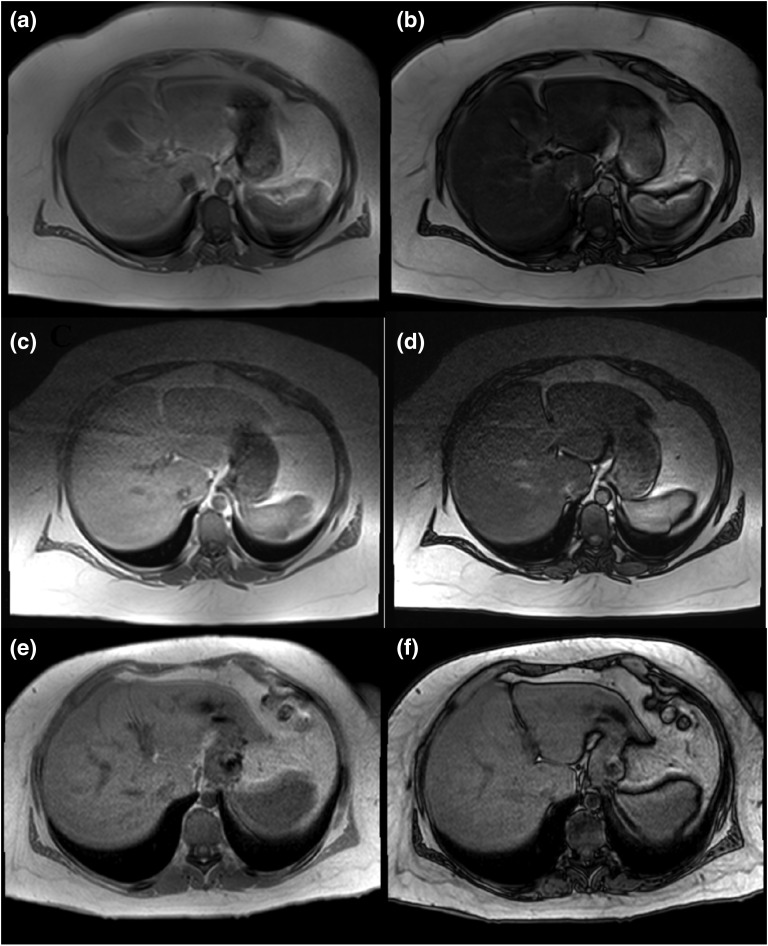
Management of adult patients with classic congenital adrenal hyperplasia (CAH) is challenging and often complicated by obesity, metabolic syndrome, and adverse cardiovascular risk. Alterations in weight can influence cortisol kinetics. A 19-year-old woman with classic CAH and morbid obesity experienced persistent elevations of androgen levels while receiving oral glucocorticoid therapy. Control of adrenal androgens was improved with continuous subcutaneous hydrocortisone infusion therapy, but obesity-related comorbidities persisted. After undergoing sleeve gastrectomy, the patient experienced dramatic weight loss, with improvement in insulin sensitivity and fatty liver in the postbariatric period. Cortisol clearance studies performed to evaluate changes in hydrocortisone dose requirements showed marked alternations in cortisol pharmacokinetics with decreases in volume of distribution and cortisol clearance, along with an increase in area under the curve for cortisol. Hydrocortisone dose was subsequently decreased 34% by 15 months after surgery. Effective control of androgen excess on this lower hydrocortisone dose was achieved and continues 27 months after surgery. This case highlights obesity-related complications of glucocorticoid replacement therapy in the management of CAH. Individual patient factors, such as fatty liver disease and insulin resistance, can have a clinically important effect on cortisol metabolism. Bariatric surgery was a safe and effective treatment of obesity in this patient with CAH and should be considered for patients with CAH and multiple obesity-related comorbidities.
成年经典型先天性肾上腺皮质增生症(CAH)患者的管理具有挑战性,且常因肥胖、代谢综合征和不良心血管风险而变得复杂。体重变化会影响皮质醇动力学。一名19岁患有经典型CAH且病态肥胖的女性在接受口服糖皮质激素治疗时雄激素水平持续升高。连续皮下输注氢化可的松治疗改善了肾上腺雄激素的控制,但肥胖相关合并症仍然存在。接受袖状胃切除术后,患者体重显著减轻,减重后胰岛素敏感性和脂肪肝情况有所改善。为评估氢化可的松剂量需求变化而进行的皮质醇清除率研究显示,皮质醇药代动力学有显著改变,分布容积和皮质醇清除率降低,同时皮质醇曲线下面积增加。术后15个月,氢化可的松剂量随后降低了34%。在较低的氢化可的松剂量下有效控制了雄激素过量,且术后27个月仍保持这种状态。该病例突出了糖皮质激素替代治疗在CAH管理中与肥胖相关的并发症。个体患者因素,如脂肪肝病和胰岛素抵抗,可对皮质醇代谢产生临床上重要的影响。减重手术是该CAH患者肥胖的一种安全有效的治疗方法,对于患有CAH和多种肥胖相关合并症的患者应考虑采用。