Centre for Molecular Imaging, Department of Cancer Imaging, Peter MacCallum Cancer Centre, 305 Grattan Street, Melbourne, Australia.
Sir Peter MacCallum Department of Oncology, University of Melbourne, 305 Grattan Street, Melbourne, Australia.
Cancer Imaging. 2017 Dec 21;17(1):31. doi: 10.1186/s40644-017-0133-5.
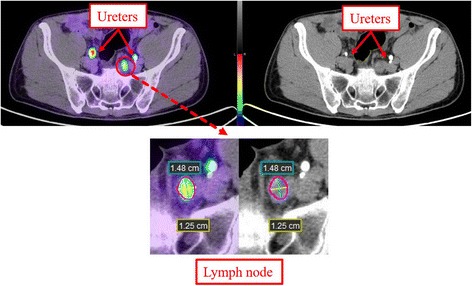
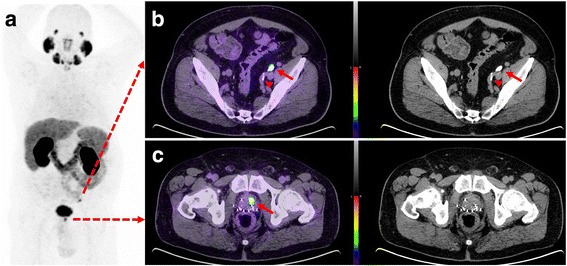
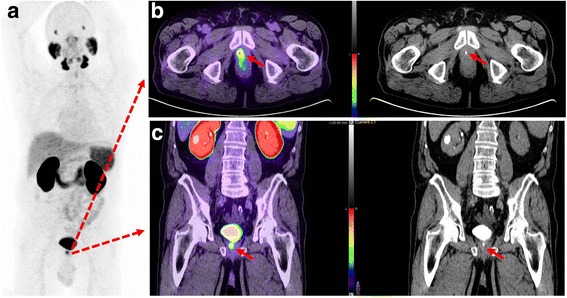
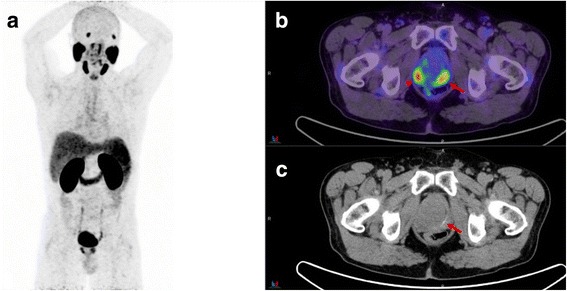
Ga-labelled prostate specific membrane antigen (PSMA) ligand PET/CT is a promising modality in primary staging (PS) and biochemical relapse (BCR) of prostate cancer (PC). However, pelvic nodes or local recurrences can be difficult to differentiate from radioactive urine. CT urography (CT-U) is an established method, which allows assessment of urological malignancies. The study presents a novel protocol of Ga-PSMA-11 PET/CT-U in PS and BCR of PC.
A retrospective review of PSMA PET/CT-U preformed on 57 consecutive patients with prostate cancer. Fifty mL of IV contrast was administered 10 min (range 8-15) before the CT component of a combined PET/CT study, acquired approximately 60 min (range 40-85) after administration of 166 MBq (range 91-246) of Ga-PSMA-11. PET and PET/CT-U were reviewed by two nuclear medicine physicians and CT-U by a radiologist. First, PET images were reviewed independently followed by PET/CT-U images. Foci of activity which could not unequivocally be assessed as disease or urinary activity were recorded. PET/CT-U was considered of potential benefit in final interpretation when the equivocal focal activity in PET images corresponded to opacified ureter, bladder, prostate bed, seminal vesicles, or urethra. Student's T test and Pearson's correlation coefficient was used for assessment of variables including lymph node size and standardized uptake value.
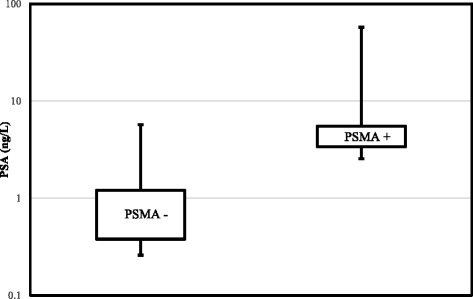
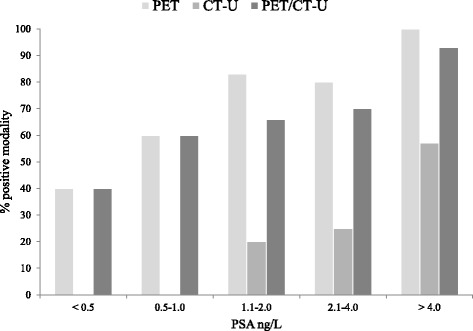
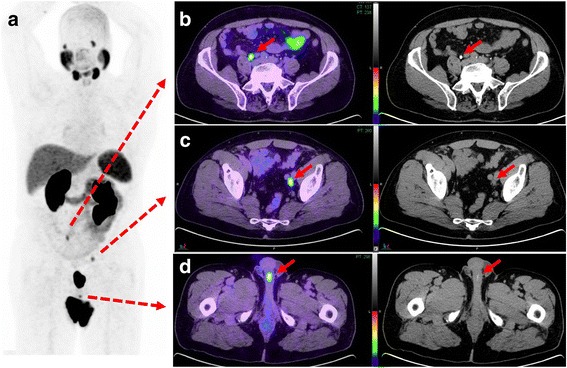
Overall 50 PSMA PET/CT-U studies were performed for BCR and 7 for PS. Median PSA with BCR and PS were 2.0 ± 11.4 ng/ml (0.06-57.3 ng/ml) and 18 ± 35.3 ng/ml (6.8-100 ng/ml), respectively. The median Gleason-score for both groups was 7 (range 6-10). In BCR group, PSMA PET was reported positive in 36 (72%) patients, CT-U in 11(22%) patients and PET/CT-U in 33 (66%) patients. In PS group, PSMA PET detected the primary site in all seven patients, of which one patient with metastatic nodal disease had negative CT finding. Of 40 equivocal foci (27/57 patients) on PET, 11 foci (10/57 patients, 17.5%) were localized to enhanced urine on PET/CT-U, hence considered of potential benefit in interpretation. Of those, 3 foci (3 patients) were solitary sites of activity on PSMA imaging including two local and one nodal site and 4 foci (3 patients) were in different nodal fields.
PET/CT-U protocol is a practical approach and may assist in interpretation of Ga-PSMA-11 imaging by delineation of the contrast opacified genitourinary system and matching focal PSMA activity with urinary contrast.
镓标记的前列腺特异性膜抗原(PSMA)配体 PET/CT 是一种有前途的方法,可用于前列腺癌(PC)的原发分期(PS)和生化复发(BCR)。然而,盆腔淋巴结或局部复发可能难以与放射性尿液区分。尿路 CT 造影(CT-U)是一种成熟的方法,可用于评估泌尿系统恶性肿瘤。本研究提出了一种新型的 Ga-PSMA-11 PET/CT-U 在 PS 和 BCR 中的应用方案。
回顾性分析了 57 例连续前列腺癌患者的 Ga-PSMA-11 PET/CT-U 检查结果。在进行 PET/CT 联合研究的 CT 成分前 10 分钟(范围 8-15 分钟)静脉注射 50ml 对比剂,在注射 166MBq(范围 91-246)Ga-PSMA-11 后约 60 分钟(范围 40-85 分钟)进行。两名核医学医师对 PET 和 PET/CT-U 进行了评估,放射科医师对 CT-U 进行了评估。首先,独立评估 PET 图像,然后评估 PET/CT-U 图像。记录无法明确评估为疾病或尿液活动的活动焦点。当 PET 图像中的可疑局灶性活性与显影的输尿管、膀胱、前列腺床、精囊或尿道相对应时,认为 PET/CT-U 对最终解释具有潜在益处。使用学生 t 检验和 Pearson 相关系数评估包括淋巴结大小和标准化摄取值在内的变量。
共有 50 例 BCR 和 7 例 PS 的患者进行了 Ga-PSMA-11 PET/CT-U 检查。BCR 和 PS 组的中位 PSA 分别为 2.0±11.4ng/ml(0.06-57.3ng/ml)和 18±35.3ng/ml(6.8-100ng/ml)。两组的中位 Gleason 评分均为 7(范围 6-10)。在 BCR 组中,36 例(72%)患者的 PSMA PET 报告为阳性,11 例(22%)患者的 CT-U 报告为阳性,33 例(66%)患者的 PET/CT-U 报告为阳性。在 PS 组中,PSMA PET 检测到了所有 7 例患者的原发性疾病,其中 1 例转移性淋巴结疾病患者的 CT 检查为阴性。在 40 个可疑病灶(57 例患者中的 27 个)中,11 个病灶(57 例患者中的 10 个,17.5%)在 PET/CT-U 上定位到增强的尿液,因此认为在解释中具有潜在益处。其中,3 个病灶(3 例患者)为 PSMA 成像中的孤立性活性部位,包括 2 个局部和 1 个淋巴结部位,4 个病灶(3 例患者)位于不同的淋巴结区域。
PET/CT-U 方案是一种实用的方法,通过描绘对比剂显影的泌尿生殖系统并将局灶性 PSMA 活性与尿路对比剂相匹配,可协助 Ga-PSMA-11 成像的解释。