Maxwell Amy E, Parker Richard A, Drever Jonathan, Rudd Anthony, Dennis Martin S, Weir Christopher J, Al-Shahi Salman Rustam
Centre for Clinical Brain Sciences, University of Edinburgh, Chancellor's Building, 49 Little France Crescent, Edinburgh, EH16 4SB, UK.
Edinburgh Clinical Trials Unit and Centre for Population Health Sciences, Usher Institute of Population Health Sciences and Informatics, University of Edinburgh, Edinburgh, UK.
Trials. 2017 Dec 28;18(1):623. doi: 10.1186/s13063-017-2355-z.
Few interventions are proven to increase recruitment in clinical trials. Recruitment to RESTART, a randomised controlled trial of secondary prevention after stroke due to intracerebral haemorrhage, has been slower than expected. Therefore, we sought to investigate an intervention to boost recruitment to RESTART.
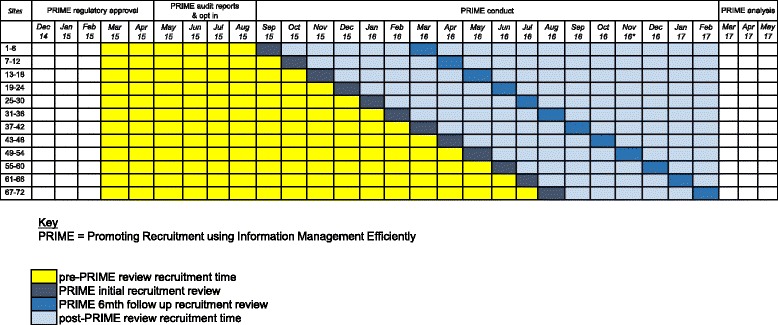
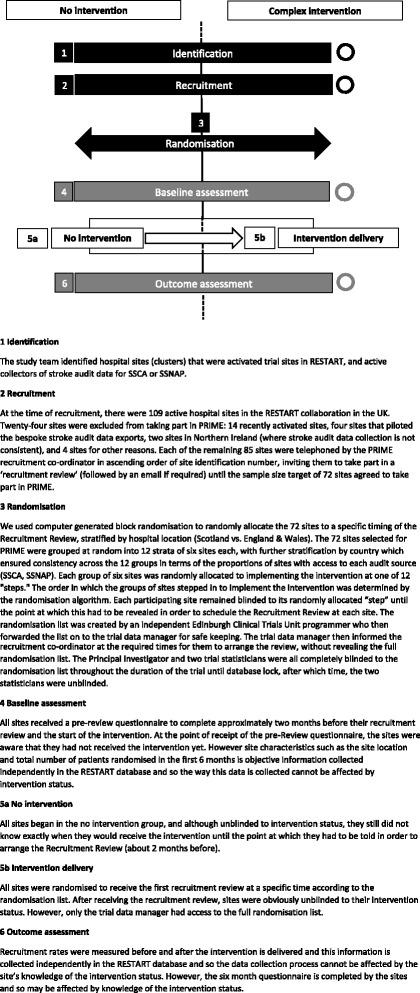
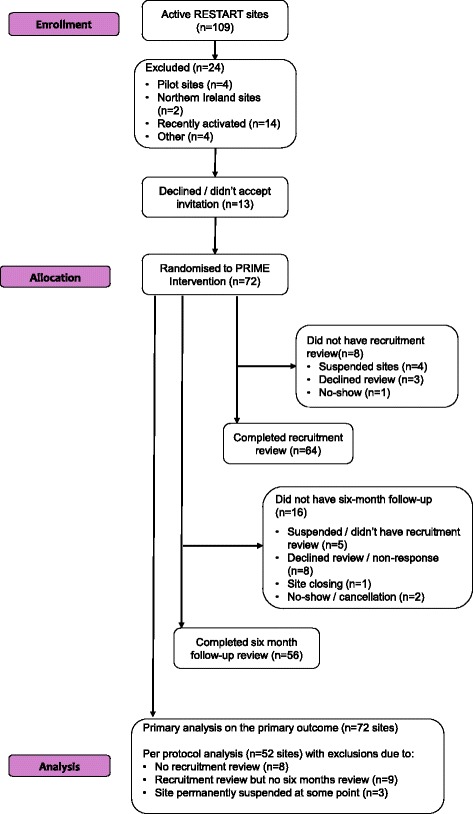
METHODS/DESIGN: We conducted a stepped-wedge, cluster randomised trial of a complex intervention to increase recruitment, embedded within the RESTART trial. The primary objective was to investigate if the PRIME complex intervention (a recruitment co-ordinator who conducts a recruitment review, provides access to bespoke stroke audit data exports, and conducts a follow-up review after 6 months) increases the recruitment rate to RESTART. We included 72 hospital sites located in England, Wales, or Scotland that were active in RESTART in June 2015. All sites began in the control state and were allocated using block randomisation stratified by hospital location (Scotland versus England/Wales) to start the complex intervention in one of 12 different months. The primary outcome was the number of patients randomised into RESTART per month per site. We quantified the effect of the complex intervention on the primary outcome using a negative binomial, mixed model adjusting for site, December/January months, site location, and background time trends in recruitment rate.
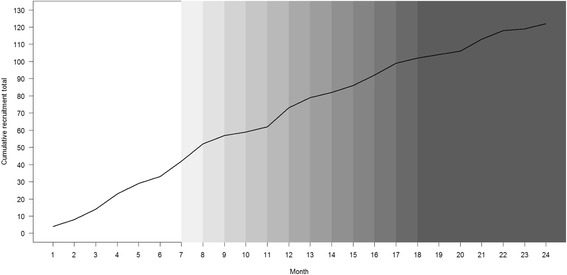
We recruited and randomised 72 sites and recorded their monthly recruitment to RESTART over 24 months (March 2015 to February 2017 inclusive), providing 1728 site-months of observations for the primary analysis. The adjusted rate ratio for the number of patients randomised per month after allocation to the PRIME complex intervention versus control time before allocation to the PRIME complex intervention was 1.06 (95% confidence interval 0.55 to 2.03, p = 0.87). Although two thirds of respondents to the 6-month follow-up questionnaire agreed that the audit reports were useful, only six patients were reported to have been randomised using the audit reports. Respondents frequently reported resource and time pressures as being key barriers to running the audit reports.
The PRIME complex intervention did not significantly improve the recruitment rate to RESTART. Further research is needed to establish if PRIME might be beneficial at an earlier stage in a prevention trial or for prevention dilemmas that arise more often in clinical practice.
很少有干预措施被证明能提高临床试验的招募率。脑出血后二级预防的随机对照试验RESTART的招募速度比预期要慢。因此,我们试图研究一种干预措施来促进RESTART的招募。
方法/设计:我们在RESTART试验中进行了一项阶梯式楔形整群随机试验,以实施一项旨在提高招募率的复杂干预措施。主要目的是研究PRIME复杂干预措施(一名招募协调员进行招募审查,提供定制的中风审计数据导出,并在6个月后进行随访审查)是否能提高RESTART的招募率。我们纳入了2015年6月在RESTART中活跃的位于英格兰、威尔士或苏格兰的72家医院。所有站点均从对照状态开始,并根据医院位置(苏格兰与英格兰/威尔士)进行分层区组随机化,以在12个不同月份中的一个开始实施复杂干预措施。主要结局是每个站点每月随机分配到RESTART的患者数量。我们使用负二项混合模型对站点、12月/1月、站点位置以及招募率的背景时间趋势进行调整,以量化复杂干预措施对主要结局的影响。
我们招募了72个站点并进行了随机分组,并记录了它们在24个月(2015年3月至2017年2月,含2月)内每月进入RESTART的招募情况,为主要分析提供了1728个站点月的观察数据。分配到PRIME复杂干预措施后每月随机分配的患者数量与分配到PRIME复杂干预措施前的对照时间相比,调整后的率比为1.06(95%置信区间0.55至2.03,p = 0.87)。尽管6个月随访问卷的三分之二受访者认为审计报告有用,但据报告只有6名患者是通过审计报告进行随机分组的。受访者经常报告资源和时间压力是运行审计报告的关键障碍。
PRIME复杂干预措施并未显著提高RESTART的招募率。需要进一步研究以确定PRIME在预防试验的早期阶段或临床实践中更常出现的预防难题中是否可能有益。