Cedars-Sinai Medical Center, 444 S. San Vicente Blvd, Suite 103, Los Angeles, CA, 90048, USA.
University of Southern California, Los Angeles, CA, USA.
Neuropsychol Rev. 2017 Dec;27(4):440-484. doi: 10.1007/s11065-017-9363-3. Epub 2017 Dec 27.
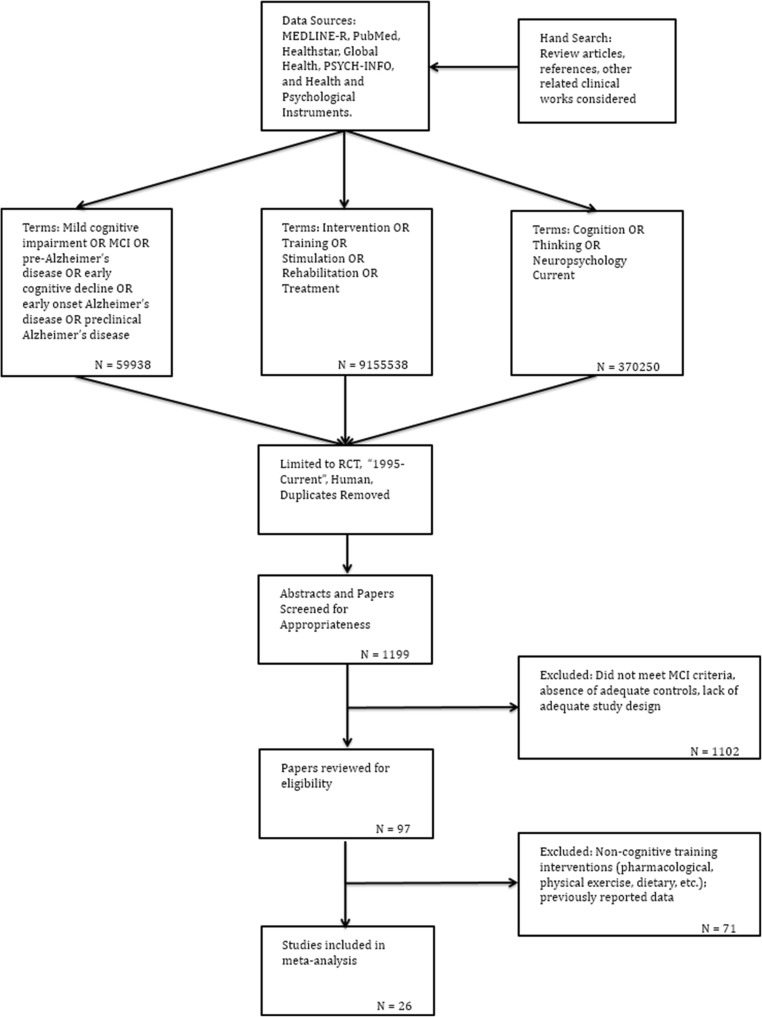
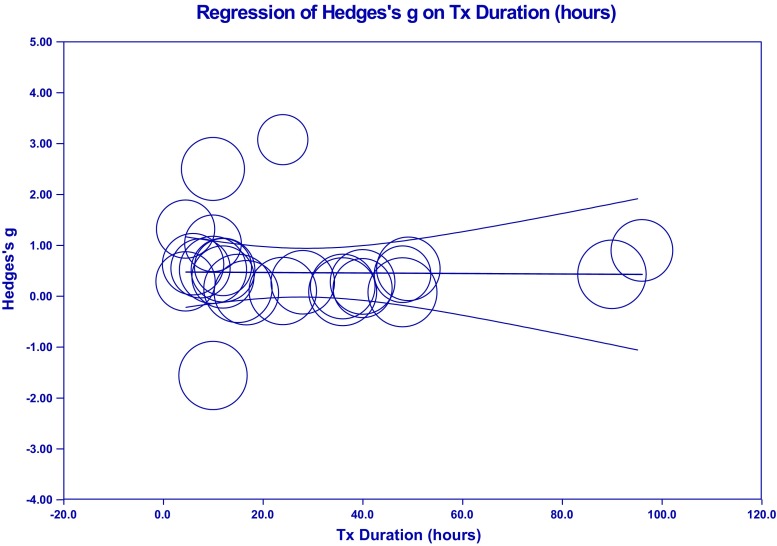
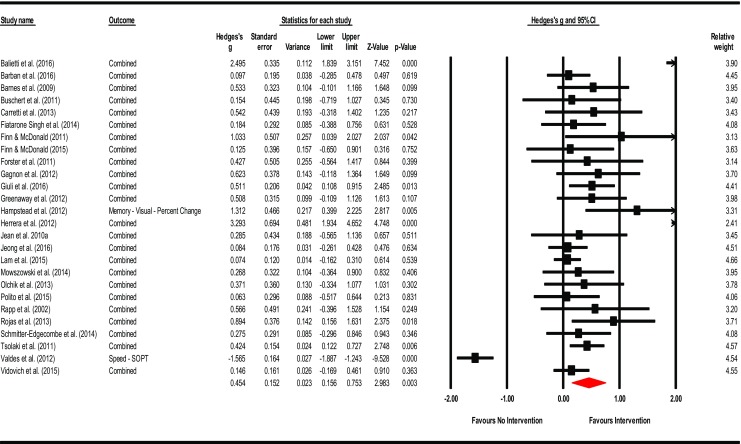
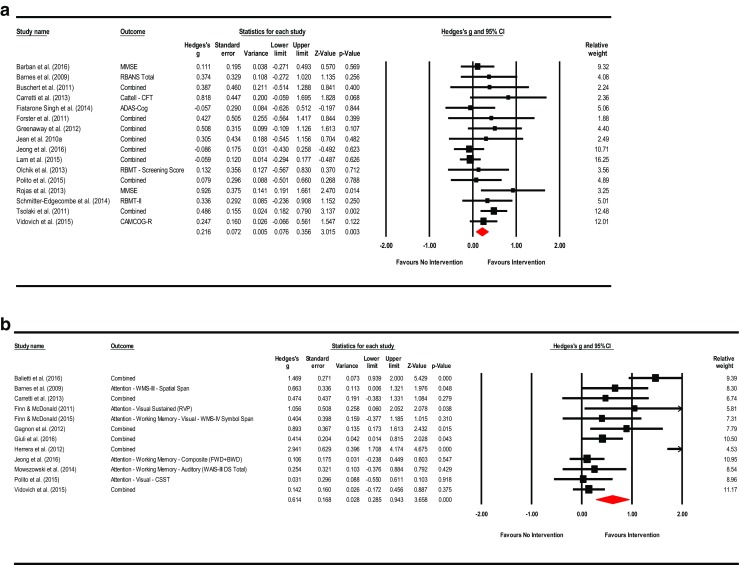
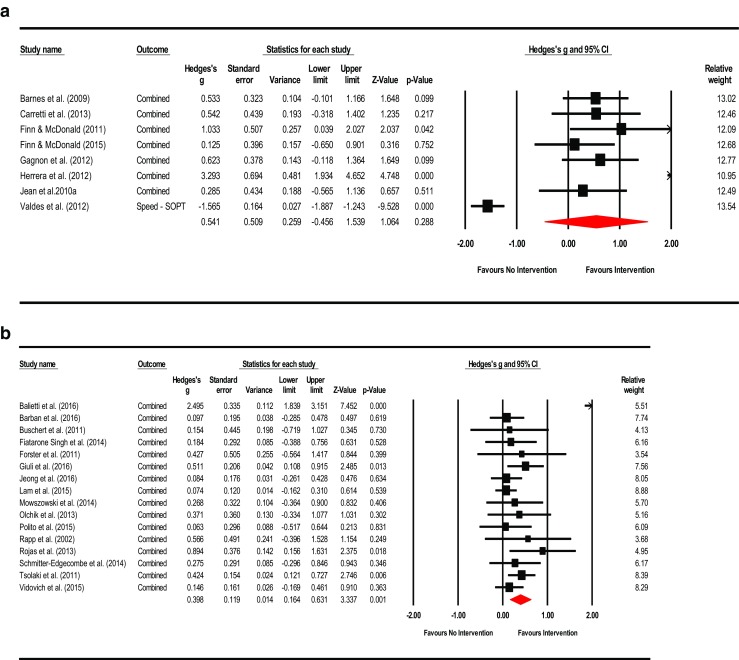
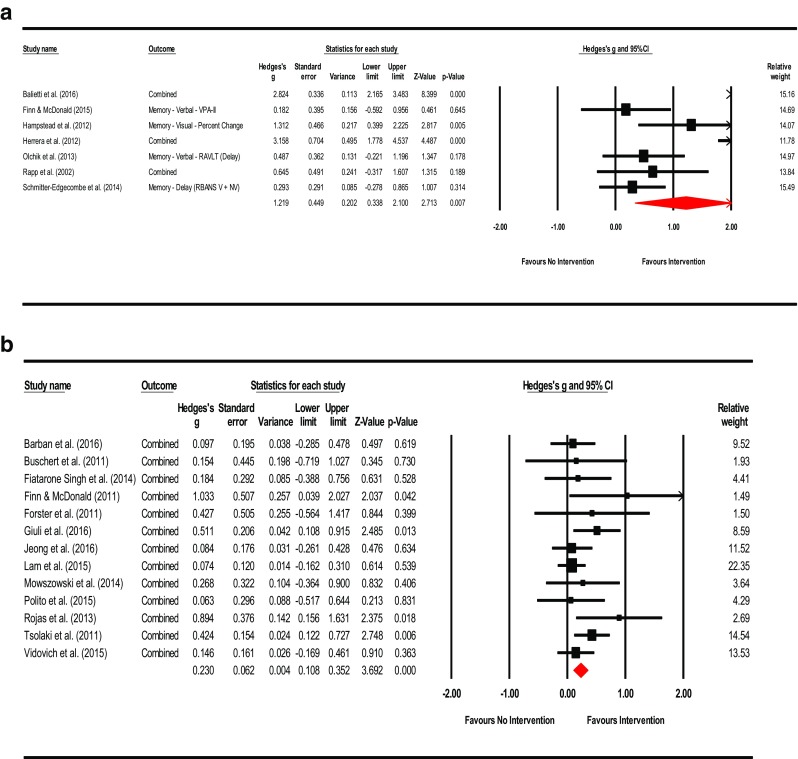
Cognitive training in MCI may stimulate pre-existing neural reserves or recruit neural circuitry as "compensatory scaffolding" prompting neuroplastic reorganization to meet task demands (Reuter-Lorenz & Park, 2014). However, existing systematic reviews and meta-analytic studies exploring the benefits of cognitive interventions in MCI have been mixed. An updated examination regarding the efficacy of cognitive intervention in MCI is needed given improvements in adherence to MCI diagnostic criteria in subject selection, better defined interventions and strategies applied, increased use of neuropsychological measures pre- and post-intervention, as well as identification of moderator variables which may influence treatment. As such, this meta-analytic review was conducted to examine the efficacy of cognitive intervention in individuals diagnosed with mild cognitive impairment (MCI) versus MCI controls based on performance of neuropsychological outcome measures in randomized controlled trials (RCT). RCT studies published from January 1995 to June 2017 were obtained through source databases of MEDLINE-R, PubMed, Healthstar, Global Health, PSYCH-INFO, and Health and Psychological Instruments using search parameters for MCI diagnostic category (mild cognitive impairment, MCI, pre-Alzheimer's disease, early cognitive decline, early onset Alzheimer's disease, and preclinical Alzheimer's disease) and the intervention or training conducted (intervention, training, stimulation, rehabilitation, or treatment). Other inclusion and exclusion criteria included subject selection based on established MCI criteria, RCT design in an outpatient setting, MCI controls (active or passive), and outcomes based on objective neuropsychological measures. From the 1199 abstracts identified, 26 articles met inclusion criteria for the meta-analyses completed across eleven (11) countries; 92.31% of which have been published within the past 7 years. A series of meta-analyses were performed to examine the effects of cognitive intervention by cognitive domain, type of training, and intervention content (cognitive domain targeted). We found significant, moderate effects for multicomponent training (Hedges' g observed = 0.398; CI [0.164, 0.631]; Z = 3.337; p = 0.001; Q = 55.511; df = 15; p = 0.000; I = 72.978%; τ = 0.146) as well as multidomain-focused strategies (Hedges' g = 0.230; 95% CI [0.108, 0.352]; Z = 3.692; p < 0.001; Q = 12.713; df = 12; p = 0.390; I = 5.612; τ = 0.003). The effects for other interventions explored by cognitive domain, training type, or intervention content were indeterminate due to concerns for heterogeneity, bias, and small cell sizes. In addition, subgroup and meta-regression analyses were conducted with the moderators of MCI category, mode of intervention, training type, intervention content, program duration (total hours), type of control group (active or passive), post-intervention follow-up assessment period, and control for repeat administration. We found significant overall effects for intervention content with memory focused interventions appearing to be more effective than multidomain approaches. There was no evidence of an influence on outcomes for the other covariates examined. Overall, these findings suggest individuals with MCI who received multicomponent training or interventions targeting multiple domains (including lifestyle changes) were apt to display an improvement on outcome measures of cognition post-intervention. As such, multicomponent and multidomain forms of intervention may prompt recruitment of alternate neural processes as well as support primary networks to meet task demands simultaneously. In addition, interventions with memory and multidomain forms of content appear to be particularly helpful, with memory-based approaches possibly being more effective than multidomain methods. Other factors, such as program duration, appear to have less of an influence on intervention outcomes. Given this, although the creation of new primary network paths appears strained in MCI, interventions with memory-based or multidomain forms of content may facilitate partial activation of compensatory scaffolding and neuroplastic reorganization. The positive benefit of memory-based strategies may also reflect transfer effects indicative of compensatory network activation and the multiple-pathways involved in memory processes. Limitations of this review are similar to other meta-analysis in MCI, including a modest number studies, small sample sizes, multiple forms of interventions and types of training applied (some overlapping), and, while greatly improved in our view, a large diversity of instruments used to measure outcome. This is apt to have contributed to the presence of heterogeneity and publication bias precluding a more definitive determination of the outcomes observed.
认知训练在 MCI 中可能会刺激预先存在的神经储备,或招募神经回路作为“代偿性支架”,从而促使神经可塑性重组以满足任务需求(Reuter-Lorenz 和 Park,2014 年)。然而,现有的系统评价和荟萃分析研究探索认知干预在 MCI 中的益处结果不一。鉴于在受试者选择中对 MCI 诊断标准的依从性有所提高,干预和策略的定义更加明确,干预前后神经心理学测量的应用增加,以及可以影响治疗的调节变量的确定,因此需要对认知干预在 MCI 中的疗效进行更新的检查。因此,进行了这项荟萃分析,以根据随机对照试验(RCT)中的神经心理学结果衡量标准,检查认知干预在轻度认知障碍(MCI)个体与 MCI 对照组中的疗效。通过 MEDLINE-R、PubMed、Healthstar、Global Health、PSYCH-INFO 和 Health and Psychological Instruments 等来源数据库,获取了从 1995 年 1 月至 2017 年 6 月发表的 RCT 研究。使用 MCI 诊断类别(轻度认知障碍、MCI、前驱期阿尔茨海默病、早期认知下降、早发性阿尔茨海默病和临床前阿尔茨海默病)和干预或训练(干预、训练、刺激、康复或治疗)的搜索参数,对 MCI 进行搜索。其他纳入和排除标准包括基于既定 MCI 标准的受试者选择、门诊环境中的 RCT 设计、MCI 对照组(主动或被动)以及基于客观神经心理学测量的结果。从确定的 1199 篇摘要中,有 26 篇文章符合完成的 11 个国家的荟萃分析纳入标准;其中 92.31%是在过去 7 年内发表的。进行了一系列荟萃分析,以检查认知干预在认知领域、训练类型和干预内容(针对的认知领域)方面的效果。我们发现,多成分训练(Hedges' g 观察值=0.398;CI [0.164, 0.631];Z=3.337;p=0.001;Q=55.511;df=15;p=0.000;I 2=72.978%;τ 2=0.146)和多领域聚焦策略(Hedges' g=0.230;95% CI [0.108, 0.352];Z=3.692;p <0.001;Q=12.713;df=12;p=0.390;I 2=5.612%;τ 2=0.003)具有显著的中度效果。由于存在异质性、偏倚和小细胞大小等问题,其他干预措施的效果不确定。此外,还进行了亚组和荟萃回归分析,以确定 MCI 类别、干预方式、训练类型、干预内容、项目持续时间(总时间)、对照组类型(主动或被动)、干预后随访评估期和重复给药的控制等调节因素的影响。我们发现,干预内容的整体效果显著,记忆为重点的干预似乎比多领域方法更有效。没有证据表明其他被检查的协变量对结果有影响。总的来说,这些发现表明,接受多成分训练或针对多个领域(包括生活方式改变)的干预的 MCI 患者在干预后认知结果测量上更有可能得到改善。因此,多成分和多领域形式的干预可能会同时激发替代神经过程,并支持主要网络满足任务需求。此外,具有记忆和多领域形式内容的干预措施似乎特别有帮助,基于记忆的方法可能比多领域方法更有效。其他因素,如项目持续时间,对干预结果的影响似乎较小。考虑到这一点,尽管在 MCI 中创建新的主要网络路径似乎很困难,但基于记忆或多领域形式的内容的干预措施可能会促进补偿性支架的部分激活和神经可塑性重组。基于记忆的策略的积极益处也可能反映出补偿性网络激活和记忆过程中涉及的多个路径的转移效应。本综述的局限性与其他 MCI 中的荟萃分析类似,包括研究数量有限、样本量小、应用的多种干预措施和类型的训练(有些重叠),以及虽然我们认为在很大程度上有所改善,但用于测量结果的仪器种类繁多。这可能导致存在异质性和发表偏倚,从而无法更明确地确定观察到的结果。