Cardiovascular Imaging Program, Departments of Medicine and Radiology, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
Center for Advanced Heart Diseases, Department of Medicine, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
Eur Heart J. 2018 Mar 7;39(10):840-849. doi: 10.1093/eurheartj/ehx721.
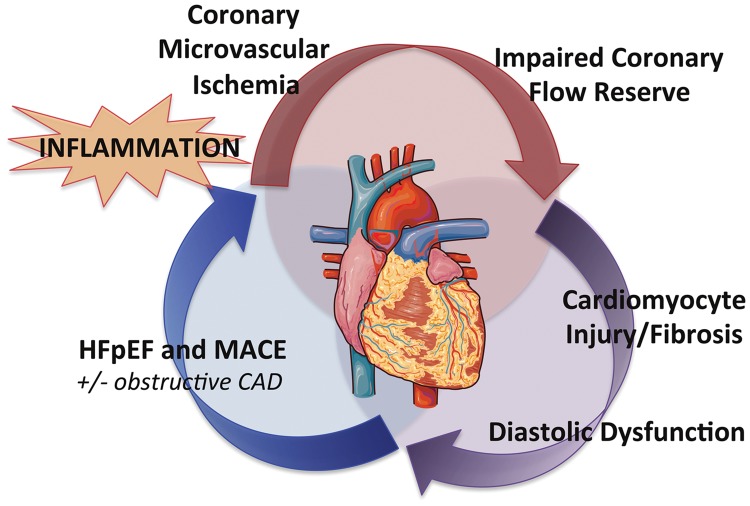
Coronary microvascular ischaemia, cardiomyocyte injury and stiffness may play an important role in the pathophysiology of heart failure with preserved ejection fraction (HFpEF). To date, the relationship between coronary flow reserve (CFR), myocardial injury, diastolic dysfunction, and future HFpEF risk is unknown.
Consecutive patients (n = 201) undergoing evaluation for suspected coronary artery disease (CAD) with stress myocardial perfusion positron emission tomography, serum troponin, and transthoracic echocardiography who did not have flow-limiting CAD or reduced left ventricular ejection fraction were identified. Patients were followed up (median 4.1 years) for cardiovascular death and hospitalization for non-fatal myocardial infarction or heart failure. Coronary flow reserve was quantified as stress/rest myocardial blood flow. Early diastolic flow (E) and relaxation (e') velocities were obtained via transmitral and tissue Doppler, respectively. Patients with impaired CFR (<2, n = 108) demonstrated linearly decreasing e' and increasing E/e' consistent with worsening diastolic function (P for trend <0.0001). A detectable troponin was associated with diastolic dysfunction only in the presence of impaired CFR (interaction P = 0.002). In adjusted analyses, impaired CFR was independently associated with diastolic dysfunction (E/e'septal > 15, adjusted OR 2.58, 95%CI 1.22-5.48) and composite cardiovascular outcomes or HFpEF hospitalization alone (adjusted HR 2.47, 95%CI 1.09-5.62). Patients with both impaired CFR and diastolic dysfunction demonstrated >five-fold increased risk of HFpEF hospitalization (P < 0.001).
In symptomatic patients without overt CAD, impaired CFR was independently associated with diastolic dysfunction and adverse events, especially HFpEF hospitalization. The presence of both coronary microvascular and diastolic dysfunctions was associated with a markedly increased risk of HFpEF events.
冠状动脉微血管缺血、心肌细胞损伤和僵硬度可能在射血分数保留的心力衰竭(HFpEF)的病理生理学中起重要作用。迄今为止,冠状动脉血流储备(CFR)、心肌损伤、舒张功能障碍与未来 HFpEF 风险之间的关系尚不清楚。
连续入选了 201 例因疑似冠心病(CAD)而行应激心肌灌注正电子发射断层扫描、血清肌钙蛋白和经胸超声心动图检查且无血流限制 CAD 或左心室射血分数降低的患者。中位随访时间为 4.1 年,随访终点为心血管死亡和非致命性心肌梗死或心力衰竭住院。通过心肌血流储备定量评估应激/静息心肌血流。通过组织多普勒获取舒张早期血流(E)和松弛(e')速度。CFR 受损(<2,n=108)的患者,随着舒张功能恶化,e'逐渐降低,E/e'逐渐升高(趋势 P<0.0001)。仅在 CFR 受损时,可检测到肌钙蛋白与舒张功能障碍相关(交互 P=0.002)。在调整分析中,CFR 受损与舒张功能障碍独立相关(间隔 E/e' > 15,调整 OR 2.58,95%CI 1.22-5.48)和复合心血管结局或单纯 HFpEF 住院(调整 HR 2.47,95%CI 1.09-5.62)。CFR 受损和舒张功能障碍的患者 HFpEF 住院风险增加>5 倍(P<0.001)。
在无症状且无明显 CAD 的患者中,CFR 受损与舒张功能障碍和不良事件,特别是 HFpEF 住院独立相关。冠状动脉微血管和舒张功能障碍的存在与 HFpEF 事件风险显著增加相关。