Pilichowska Monika, Pittaluga Stefania, Ferry Judith A, Hemminger Jessica, Chang Hong, Kanakry Jennifer A, Sehn Laurie H, Feldman Tatyana, Abramson Jeremy S, Kritharis Athena, Hernandez-Ilizaliturri Francisco J, Lossos Izidore S, Press Oliver W, Fenske Timothy S, Friedberg Jonathan W, Vose Julie M, Blum Kristie A, Jagadeesh Deepa, Woda Bruce, Gupta Gaurav K, Gascoyne Randy D, Jaffe Elaine S, Evens Andrew M
Department of Pathology and Laboratory Medicine, Tufts Medical Center, Boston, MA.
Laboratory of Pathology, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD.
Blood Adv. 2017 Dec 11;1(26):2600-2609. doi: 10.1182/bloodadvances.2017009472. eCollection 2017 Dec 12.
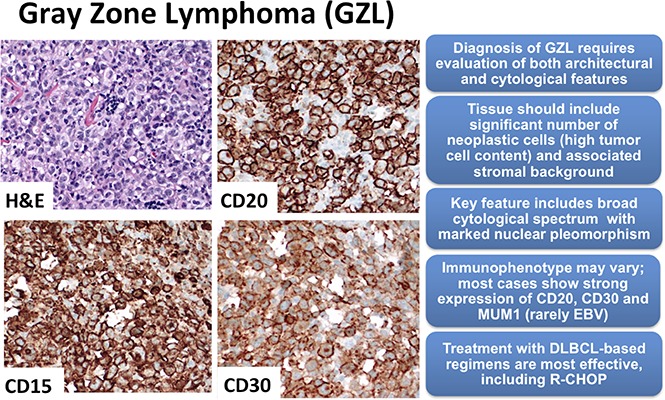
Gray zone lymphoma (GZL) is described as sharing features with classical Hodgkin lymphoma (cHL) and diffuse large B-cell lymphoma (DLBCL). However, there remains complexity in establishing diagnosis, delineating prognosis, and determining optimum therapy. Sixty-eight cases diagnosed as GZL across 15 North American academic centers were evaluated by central pathology review to achieve consensus. Of these, only 26 (38%) were confirmed as GZL. Morphology was critical to GZL consensus diagnosis (eg, tumor cell richness); immunohistochemistry showed universal B-cell derivation, frequent CD30 expression, and rare Epstein-Barr virus (EBV) positivity (CD20, 83%; PAX5, 100%; BCL6, 20%; MUM1, 100%; CD30, 92%; EBV, 4%). Forty-two cases were reclassified: nodular sclerosis (NS) cHL, n = 27 (including n = 10 NS grade 2); lymphocyte predominant HL, n = 4; DLBCL, n = 4; EBV DLBCL, n = 3; primary mediastinal large BCL n = 2; lymphocyte-rich cHL and BCL-not otherwise specified, n = 1 each. GZL consensus-confirmed vs reclassified cases, respectively, more often had mediastinal disease (69% vs 41%; .038) and less likely more than 1 extranodal site (0% vs 25%; .019). With a 44-month median follow-up, 3-year progression-free survival (PFS) and overall survival for patients with confirmed GZL were 39% and 95%, respectively, vs 58% and 85%, respectively, for reclassified cases ( .19 and .15, respectively). Interestingly, NS grade 2 reclassified patients had similar PFS as GZL consensus-confirmed cases. For prognostication of GZL cases, hypoalbuminemia was a negative factor (3-year PFS, 12% vs 64%; = .01), whereas frontline cyclophosphamide, doxorubicin, vincristine, and prednisone ± rituximab (CHOP±R) was associated with improved 3-year PFS (70% vs 20%; .03); both factors remained significant on multivariate analysis. Altogether, accurate diagnosis of GZL remains challenging, and improved therapeutic strategies are needed.
灰色地带淋巴瘤(GZL)被描述为具有与经典霍奇金淋巴瘤(cHL)和弥漫性大B细胞淋巴瘤(DLBCL)相同的特征。然而,在确立诊断、描述预后和确定最佳治疗方案方面仍存在复杂性。15个北美学术中心诊断为GZL的68例病例经中心病理复查以达成共识。其中,仅26例(38%)被确认为GZL。形态学对GZL的共识诊断至关重要(例如,肿瘤细胞丰富度);免疫组化显示均为B细胞来源,CD30表达频繁,而爱泼斯坦-巴尔病毒(EBV)阳性罕见(CD20,83%;PAX5,100%;BCL6,20%;MUM1,100%;CD30,92%;EBV,4%)。42例病例被重新分类:结节硬化型(NS)cHL,n = 27(包括n = 10例2级NS);淋巴细胞为主型HL,n = 4;DLBCL,n = 4;EBV DLBCL,n = 3;原发性纵隔大B细胞淋巴瘤,n = 2;富于淋巴细胞的cHL和未另行指定的B细胞淋巴瘤,各n = 1。经GZL共识确认病例与重新分类病例相比,更常出现纵隔疾病(69%对41%;P = 0.038),且出现超过1个结外部位的可能性较小(0%对25%;P = 0.019)。中位随访44个月时,确诊为GZL患者的3年无进展生存期(PFS)和总生存期分别为39%和95%,而重新分类病例分别为58%和85%(P分别为0.19和0.15)。有趣的是,重新分类的2级NS患者的PFS与经GZL共识确认病例相似。对于GZL病例的预后评估,低白蛋白血症是一个负面因素(3年PFS,12%对64%;P = 0.01),而一线使用环磷酰胺、阿霉素、长春新碱和泼尼松±利妥昔单抗(CHOP±R)与3年PFS改善相关(70%对20%;P = 0.03);在多变量分析中这两个因素仍然具有显著性。总之,GZL的准确诊断仍然具有挑战性,需要改进治疗策略。