Veterans Affairs Health Economics Resource Center, VA Palo Alto Health Care System, Menlo Park, California.
Veterans Affairs Center for Innovation to Implementation, Menlo Park, California.
JAMA Cardiol. 2018 Feb 1;3(2):133-141. doi: 10.1001/jamacardio.2017.4843.
The Veterans Affairs (VA) Community Care (CC) Program supplements VA care with community-based medical services. However, access gains and value provided by CC have not been well described.
To compare the access, cost, and quality of elective coronary revascularization procedures between VA and CC hospitals and to evaluate if procedural volume or publicly reported quality data can be used to identify high-value care.
DESIGN, SETTING, AND PARTICIPANTS: Observational cohort study of veterans younger than 65 years undergoing an elective coronary revascularization, controlling for differences in risk factors using propensity adjustment. The setting was VA and CC hospitals. Participants were veterans undergoing elective percutaneous coronary intervention (PCI) and veterans undergoing coronary artery bypass graft (CABG) procedures between October 1, 2008, and September 30, 2011. The analysis was conducted between July 2014 and July 2017.
Receipt of an elective coronary revascularization at a VA vs CC facility.
Access to care as measured by travel distance, 30-day mortality, and costs.
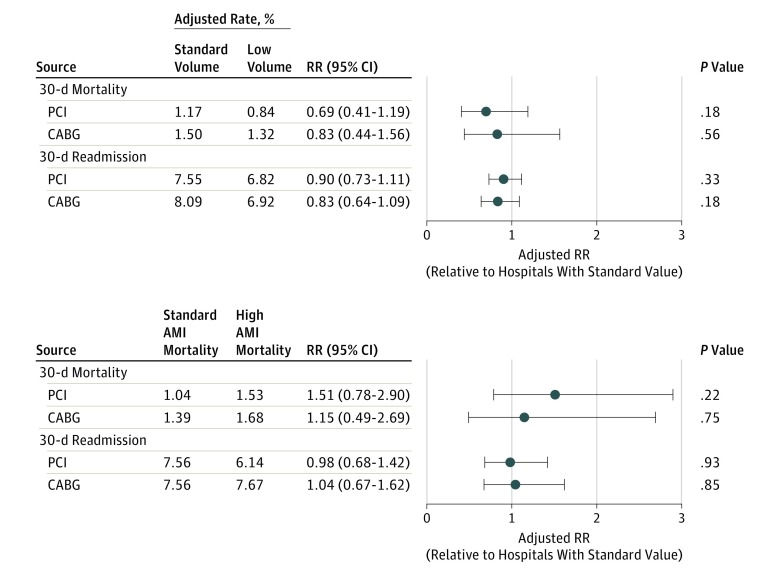
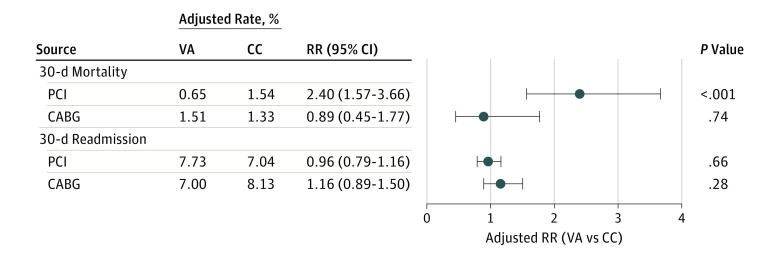
In the 3 years ending on September 30, 2011, a total of 13 237 elective PCIs (79.1% at the VA) and 5818 elective CABG procedures (83.6% at the VA) were performed in VA or CC hospitals among veterans meeting study inclusion criteria. On average, use of CC was associated with reduced net travel by 53.6 miles for PCI and by 73.3 miles for CABG surgery compared with VA-only care. Adjusted 30-day mortality after PCI was higher in CC compared with VA (1.54% for CC vs 0.65% for VA, P < .001) but was similar after CABG surgery (1.33% for CC vs 1.51% for VA, P = .74). There were no differences in adjusted 30-day readmission rates for PCI (7.04% for CC vs 7.73% for VA, P = .66) or CABG surgery (8.13% for CC vs 7.00% for VA, P = .28). The mean adjusted PCI cost was higher in CC ($22 025 for CC vs $15 683 for VA, P < .001). The mean adjusted CABG cost was lower in CC ($55 526 for CC vs $63 144 for VA, P < .01). Neither procedural volume nor publicly reported mortality data identified hospitals that provided higher-value care with the exception that CABG mortality was lower in small-volume CC hospitals.
In this veteran cohort, PCIs performed in CC hospitals were associated with shorter travel distance but with higher mortality, higher costs, and minimal travel savings compared with VA hospitals. The CABG procedures performed in CC hospitals were associated with shorter travel distance, similar mortality, and lower costs. As the VA considers expansion of the CC program, ongoing assessments of value and access gains are essential to optimize veteran outcomes and VA spending.
重要性:退伍军人事务部(VA)社区关怀(CC)计划通过基于社区的医疗服务来补充 VA 护理。然而,CC 提供的获取途径和价值尚未得到很好的描述。
目的:比较 VA 和 CC 医院进行选择性冠状动脉血运重建手术的可及性、成本和质量,并评估程序量或公开报告的质量数据是否可用于识别高价值的护理。
设计、地点和参与者:这是一项对 65 岁以下接受选择性冠状动脉血运重建的退伍军人进行的观察性队列研究,通过倾向调整来控制危险因素的差异。研究地点为 VA 和 CC 医院。参与者为接受经皮冠状动脉介入治疗(PCI)的退伍军人和接受冠状动脉旁路移植术(CABG)的退伍军人,时间为 2008 年 10 月 1 日至 2011 年 9 月 30 日。分析于 2014 年 7 月至 2017 年 7 月进行。
暴露:在 VA 与 CC 设施接受选择性冠状动脉血运重建。
主要结果和措施:可及性的衡量指标包括旅行距离、30 天死亡率和成本。
结果:在截至 2011 年 9 月 30 日的 3 年中,在符合研究纳入标准的退伍军人中,共有 13237 例选择性 PCI(79.1%在 VA)和 5818 例选择性 CABG 手术(83.6%在 VA)在 VA 或 CC 医院进行。平均而言,与仅在 VA 接受治疗相比,使用 CC 可减少 53.6 英里的净旅行距离,用于 PCI 手术,减少 73.3 英里的净旅行距离,用于 CABG 手术。与 VA 相比,CC 术后 30 天的死亡率更高(CC 为 1.54%,VA 为 0.65%,P<0.001),但 CABG 手术后的死亡率相似(CC 为 1.33%,VA 为 1.51%,P=0.74)。PCI(CC 为 7.04%,VA 为 7.73%,P=0.66)或 CABG 手术(CC 为 8.13%,VA 为 7.00%,P=0.28)后 30 天的再入院率无差异。CC 的平均调整后 PCI 成本较高(CC 为 22025 美元,VA 为 15683 美元,P<0.001)。CC 的平均调整后 CABG 成本较低(CC 为 55026 美元,VA 为 63144 美元,P<0.01)。既没有程序量,也没有公开报告的死亡率数据可以确定提供更高价值护理的医院,除了小容量 CC 医院的 CABG 死亡率较低。
结论和相关性:在这个退伍军人队列中,与 VA 医院相比,CC 医院进行的 PCI 手术与较短的旅行距离相关,但与 VA 医院相比,死亡率更高、成本更高、旅行节省最小。在 CC 医院进行的 CABG 手术与较短的旅行距离、相似的死亡率和较低的成本相关。随着 VA 考虑扩大 CC 计划,对价值和获取途径的收益进行持续评估对于优化退伍军人的结果和 VA 的支出至关重要。