Population Health Sciences, Bristol Medical School, University of Bristol, Bristol, UK.
Pakistan Health Research Council, Islamabad, Pakistan.
Int J Epidemiol. 2018 Apr 1;47(2):550-560. doi: 10.1093/ije/dyx270.
The World Health Organization (WHO) has developed a global health strategy to eliminate viral hepatitis. We project the treatment and prevention requirements to achieve the WHO HCV elimination target of reducing HCV incidence by 80% and HCV-related mortality by 65% by 2030 in Pakistan, which has the second largest HCV burden worldwide.
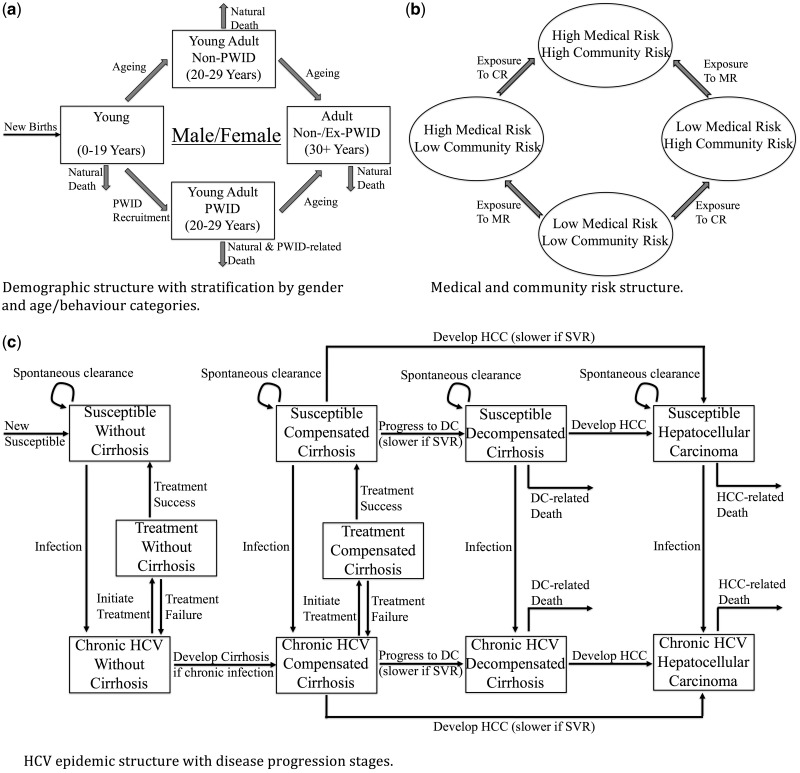
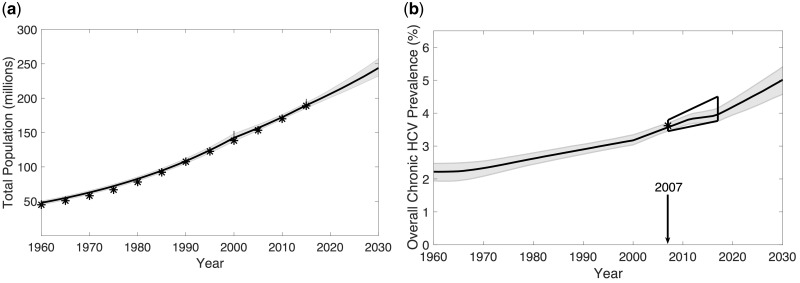
We developed an HCV transmission model for Pakistan, and calibrated it to epidemiological data from a national survey (2007), surveys among people who inject drugs (PWID), and blood donor data. Current treatment coverage data came from expert opinion and published reports. The model projected the HCV burden, including incidence, prevalence and deaths through 2030, and estimated the impact of varying prevention and direct-acting antiviral (DAA) treatment interventions necessary for achieving the WHO HCV elimination targets.
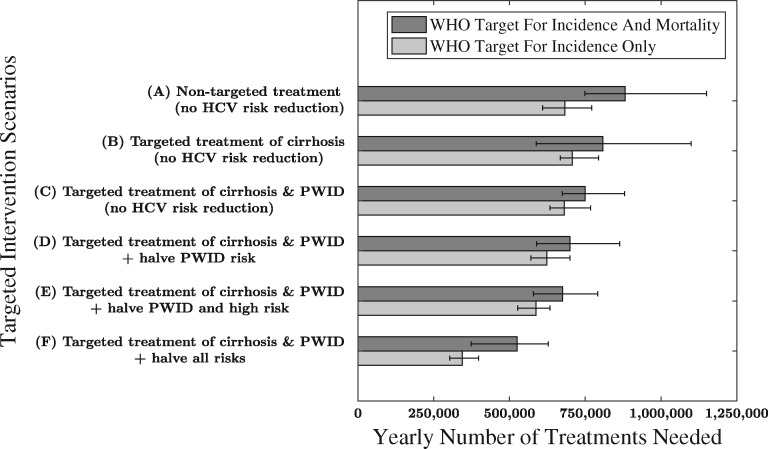
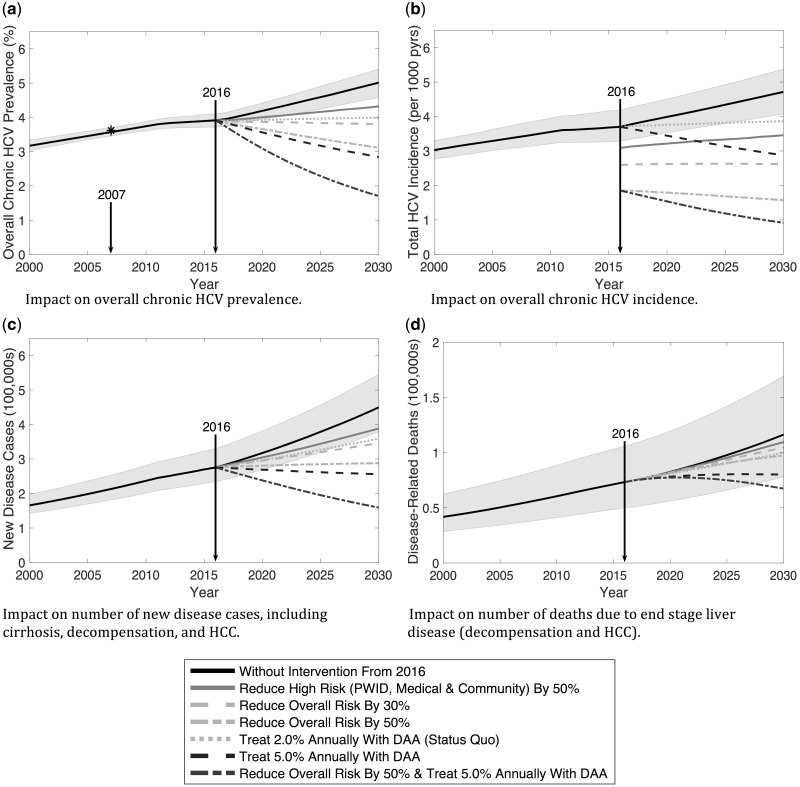
With no further treatment (currently ∼150 000 treated annually) during 2016-30, chronic HCV prevalence will increase from 3.9% to 5.1%, estimated annual incident infections will increase from 700 000 to 1 100 000, and 1 400 000 HCV-associated deaths will occur. To reach the WHO HCV elimination targets by 2030, 880 000 annual DAA treatments are required if prevention is not scaled up and no treatment prioritization occurs. By targeting treatment toward persons with cirrhosis (80% treated annually) and PWIDs (double the treatment rate of non-PWIDs), the required annual treatment number decreases to 750 000. If prevention activities also halve transmission risk, this treatment number reduces to 525 000 annually.
Substantial HCV prevention and treatment interventions are required to reach the WHO HCV elimination targets in Pakistan, without which Pakistan's HCV burden will increase markedly.
世界卫生组织(WHO)制定了一项全球卫生战略,以消除病毒性肝炎。我们预测了在巴基斯坦实现 2030 年世卫组织 HCV 消除目标(即 HCV 发病率降低 80%,相关死亡率降低 65%)所需的治疗和预防要求,该国是全球 HCV 负担第二大的国家。
我们为巴基斯坦开发了 HCV 传播模型,并根据全国性调查(2007 年)、注射吸毒者(PWID)调查和献血者数据对其进行了校准。当前的治疗覆盖率数据来自专家意见和已发表的报告。该模型预测了 2030 年之前 HCV 负担,包括发病率、患病率和死亡率,并估计了为实现世卫组织 HCV 消除目标而需要采取的不同预防和直接作用抗病毒(DAA)治疗干预措施的影响。
如果在 2016 年至 2030 年期间不进一步进行治疗(目前每年约有 15 万人接受治疗),慢性 HCV 流行率将从 3.9%上升至 5.1%,估计每年新发病例将从 70 万例增加到 110 万例,将有 140 万例 HCV 相关死亡。如果不扩大预防规模且不对治疗进行优先排序,要在 2030 年实现世卫组织 HCV 消除目标,每年需要进行 88 万例 DAA 治疗。如果将治疗目标针对肝硬化患者(每年 80%接受治疗)和 PWIDs(非 PWIDs 的治疗率加倍),则所需的年度治疗人数将减少到 75 万例。如果预防活动也将传播风险减半,那么每年的治疗人数将减少到 52.5 万例。
为了在巴基斯坦实现世卫组织 HCV 消除目标,需要采取大量 HCV 预防和治疗干预措施,否则该国的 HCV 负担将显著增加。