Beaton Dorcas E, Mamdani Muhammad, Zheng Hong, Jaglal Susan, Cadarette Suzanne M, Bogoch Earl R, Sale Joanna E M, Sujic Rebeka, Jain Ravi
Musculoskeletal Health and Outcomes Research, Li Ka Shing Knowledge Institute of St. Michael's Hospital Institute of Health Policy, Management and Evaluation, University of Toronto Occupational Sciences and Occupational Therapy, University of Toronto Institute for Work & Health Li Ka Shing Centre for Healthcare Analytics Research & Training, Li Ka Shing Knowledge Institute of St. Michael's Hospital Institute for Clinical Evaluative Sciences Leslie Dan Faculty of Pharmacy, University of Toronto Toronto Rehabilitation Institute, University Health Network Department of Physical Therapy, University of Toronto Division of Orthopaedic Surgery, Department of Surgery, University of Toronto Ontario Osteoporosis Strategy, Osteoporosis Canada, Toronto, ON, Canada.
Medicine (Baltimore). 2017 Dec;96(48):e9012. doi: 10.1097/MD.0000000000009012.
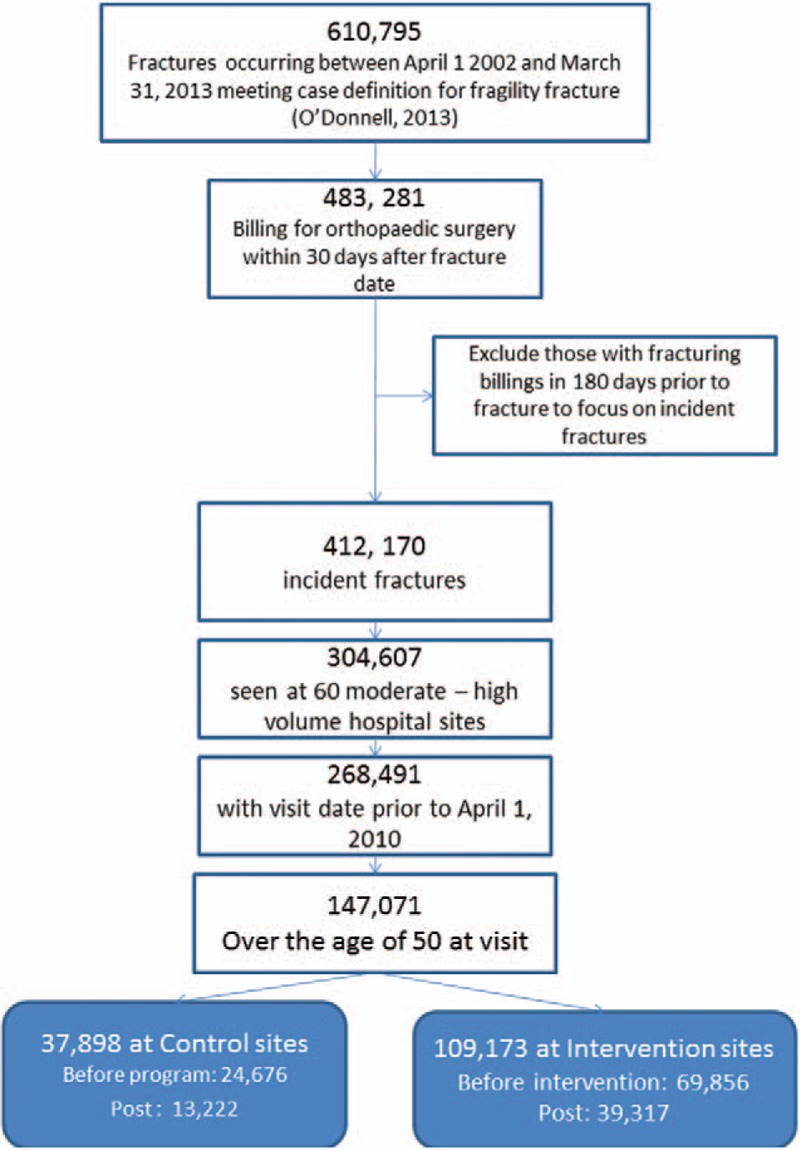
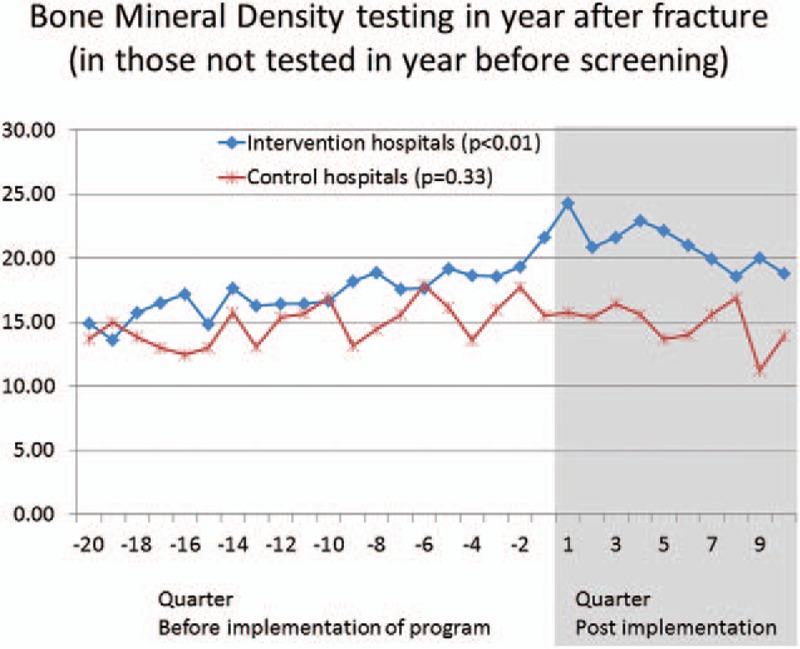
We evaluated a system-wide impact of a health intervention to improve treatment of osteoporosis after a fragility fracture. The intervention consisted of assigning a screening coordinator to selected fracture clinics to identify, educate, and follow up with fragility fracture patients and inform their physicians of the need to evaluate bone health. Thirty-seven hospitals in the province of Ontario (Canada) were assigned a screening coordinator. Twenty-three similar hospitals were control sites. All hospitals had orthopedic services and handled moderate-to-higher volumes of fracture patients. Administrative health data were used to evaluate the impact of the intervention.Fragility fracture patients (≥50 years; hip, humerus, forearm, spine, or pelvis fracture) were identified from administrative health records. Cases were fractures treated at 1 of the 37 hospitals assigned a coordinator. Controls were the same types of fractures at the control sites. Data were assembled for 20 quarters before and 10 quarters after the implementation (from January 2002 to March 2010). To test for a shift in trends, we employed an interrupted time series analysis-a study design used to evaluate the longitudinal effects of interventions, through regression modelling. The primary outcome measure was bone mineral density (BMD) testing. Osteoporosis medication initiation and persistence rates were secondary outcomes in a subset of patients ≥66 years of age.A total of 147,071 patients were used in the analysis. BMD testing rates increased from 17.0% pre-intervention to 20.9% post-intervention at intervention sites (P < .01) compared with no change at control sites (14.9% and 14.9%, P = .33). Medication initiation improved significantly at intervention sites (21.6-23.97%; P = .02) but not at control sites (17.5-18.5%; P = .27). Persistence with bisphosphonates decreased at all sites, from 59.9% to 56.4% at intervention sites (P = .02) and more so from 62.3% to 54.2% at control sites (P < .01) using 50% proportion of days covered (PDC 50).Significant improvements in BMD testing and treatment initiation were observed after the initiation of a coordinator-based screening program to improve osteoporosis management following fragility fracture.
我们评估了一项健康干预措施对改善脆性骨折后骨质疏松症治疗的全系统影响。该干预措施包括为选定的骨折诊所安排一名筛查协调员,以识别、教育和随访脆性骨折患者,并告知其医生评估骨骼健康的必要性。加拿大安大略省的37家医院被分配了一名筛查协调员。23家类似的医院作为对照站点。所有医院都提供骨科服务,且处理中高数量的骨折患者。利用行政卫生数据评估干预措施的影响。从行政卫生记录中识别出脆性骨折患者(≥50岁;髋部、肱骨、前臂、脊柱或骨盆骨折)。病例为在被分配协调员的37家医院之一接受治疗的骨折患者。对照为对照站点的相同类型骨折。在实施前的20个季度和实施后的10个季度(从2002年1月至2010年3月)收集数据。为了检验趋势的变化,我们采用了中断时间序列分析——一种通过回归建模来评估干预措施纵向影响的研究设计。主要结局指标是骨密度(BMD)检测。骨质疏松症药物起始和持续率是≥66岁患者亚组的次要结局。
分析共纳入147,071名患者。干预站点的BMD检测率从干预前的17.0%增至干预后的20.9%(P<0.01),而对照站点无变化(分别为14.9%和14.9%,P = 0.33)。干预站点的药物起始情况显著改善(从21.6%至23.97%;P = 0.02),而对照站点未改善(从17.5%至18.5%;P = 0.27)。所有站点使用50%覆盖天数比例(PDC 50)时,双膦酸盐的持续率均下降,干预站点从59.9%降至56.4%(P = 0.02),对照站点下降幅度更大,从62.3%降至54.2%(P<0.01)。
在启动基于协调员的筛查项目以改善脆性骨折后的骨质疏松症管理后,观察到BMD检测和治疗起始情况有显著改善。