Delsuc Claire, Faure Alexandre, Berthiller Julien, Dorez Didier, Matillon Xavier, Meas-Yedid Vannary, Floccard Bernard, Marcotte Guillaume, Labeye Vanessa, Rabeyrin Maud, Codas Ricardo, Chauvet Cécile, Robinson Philip, Morelon Emmanuel, Badet Lionel, Hanf William, Rimmelé Thomas
Hospices Civils de Lyon, Hôpital Edouard Herriot, Université Claude Bernard Lyon 1, service d'Anesthésie Réanimation, Lyon, France.
EA 7426 (Université Claude Bernard Lyon 1 - Hospices Civils de Lyon - bioMérieux) "Pathophysiology of Injury-Induced Immunosuppression - PI3", Lyon, France.
BMC Nephrol. 2018 Jan 8;19(1):3. doi: 10.1186/s12882-017-0805-1.
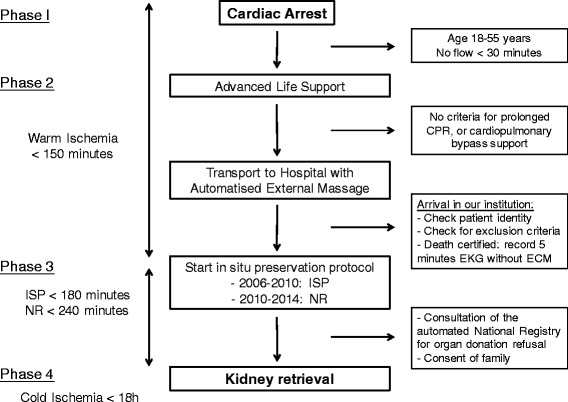
Kidney transplantation following uncontrolled donation after circulatory death (uDCD) presents a high risk of delayed graft function due to prolonged warm ischemia time. In order to minimise the effects of ischemia/reperfusion injury during warm ischemia, normothermic recirculation recently replaced in situ perfusion prior to implantation in several institutions. The aim of this study was to compare these preservation methods on kidney graft outcomes.
The primary endpoint was the one-year measured graft filtration rate (mGFR). We collected retrospective data from 64 consecutive uDCD recipients transplanted over a seven-year period in a single centre.
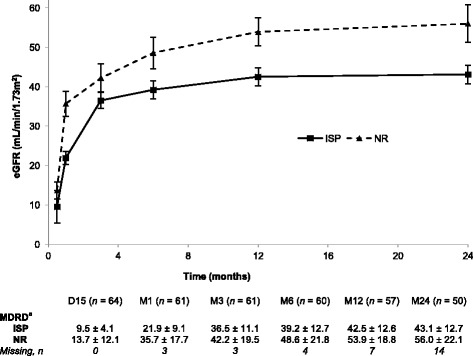
Thirty-two grafts were preserved by in situ perfusion and 32 by normothermic recirculation. The mean ± SD mGFR at 1 year post-transplantation was 43.0 ± 12.8 mL/min/1.73 m in the in situ perfusion group and 53.2 ± 12.8 mL/min/1.73 m in the normothermic recirculation group (p = 0.01). Estimated GFR levels were significantly higher in the normothermic recirculation group at 12 months (p = 0.01) and 24 months (p = 0.03) of follow-up. We did not find any difference between groups regarding patient and graft survival, delayed graft function, graft rejection, or interstitial fibrosis.
Function of grafts preserved by normothermic recirculation was better at 1 year and the results suggest that this persists at 2 years, although no difference was found in short-term outcomes. Despite the retrospective design, this study provides an additional argument in favour of normothermic recirculation.
在循环性死亡后进行非受控捐赠(uDCD)后的肾移植,由于热缺血时间延长,存在移植肾功能延迟恢复的高风险。为了尽量减少热缺血期间缺血/再灌注损伤的影响,最近在几家机构中,常温再灌注取代了植入前的原位灌注。本研究的目的是比较这些保存方法对肾移植结果的影响。
主要终点是移植肾一年测量的肾小球滤过率(mGFR)。我们收集了在一个中心7年期间连续移植的64例uDCD受者的回顾性数据。
32例移植肾通过原位灌注保存,32例通过常温再灌注保存。原位灌注组移植后1年的平均±标准差mGFR为43.0±12.8 mL/min/1.73m²,常温再灌注组为53.2±12.8 mL/min/1.73m²(p = 0.01)。在随访的12个月(p = 0.01)和24个月(p = 0.03)时,常温再灌注组的估计肾小球滤过率水平显著更高。在患者和移植肾存活、移植肾功能延迟恢复、移植肾排斥或间质纤维化方面,我们未发现两组之间存在任何差异。
常温再灌注保存的移植肾在1年时功能更好,结果表明这种情况在2年时仍然存在,尽管在短期结果中未发现差异。尽管本研究为回顾性设计,但它为支持常温再灌注提供了额外的论据。