Kortz Teresa Bleakly, Sawe Hendry R, Murray Brittany, Enanoria Wayne, Matthay Michael Anthony, Reynolds Teri
Division of Critical Care, Department of Pediatrics, University of California, San Francisco, San Francisco, CA, United States.
Institute for Global Health Sciences, University of California, San Francisco, San Francisco, CA, United States.
Front Pediatr. 2017 Dec 22;5:278. doi: 10.3389/fped.2017.00278. eCollection 2017.
Pediatric sepsis causes significant global morbidity and mortality and low- and middle-income countries (LMICs) bear the bulk of the burden. International sepsis guidelines may not be relevant in LMICs, especially in sub-Saharan Africa (SSA), due to resource constraints and population differences. There is a critical lack of pediatric sepsis data from SSA, without which accurate risk stratification tools and context-appropriate, evidence-based protocols cannot be developed. The study's objectives were to characterize pediatric sepsis presentations, interventions, and outcomes in a public Emergency Medicine Department (EMD) in Tanzania.
Prospective descriptive study of children (28 days to 14 years) with sepsis [suspected infection with ≥2 clinical systemic inflammatory response syndrome (SIRS) criteria] presenting to a tertiary EMD in Dar es Salaam, Tanzania (July 1 to September 30, 2016). Outcomes included: in-hospital mortality (primary), EMD mortality, and hospital length of stay. We report descriptive statistics using means and SDs, medians and interquartile ranges, and counts and percentages as appropriate. Predictive abilities of SIRS criteria, the Alert-Verbal-Painful-Unresponsive (AVPU) score and the Lambaréné Organ Dysfunction Score (LODS) for in-hospital, early and late mortality were tested.
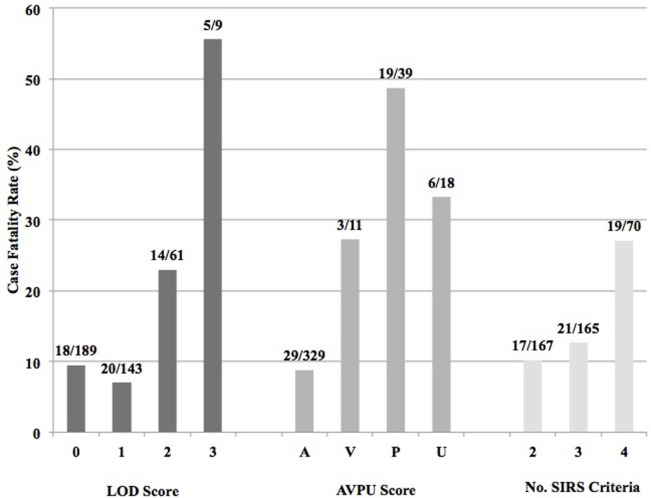
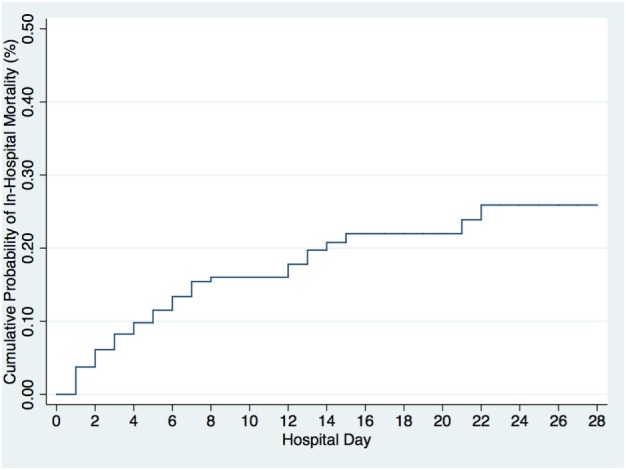
Of the 2,232 children screened, 433 (19.4%) met inclusion criteria, and 405 were enrolled. There were 247 (61%) subjects referred from an outside facility. Approximately half (54.1%) received antibiotics in the EMD, and some form of microbiologic culture was collected in 35.8% ( = 145) of subjects. In-hospital and EMD mortality were 14.2 and 1.5%, respectively, median time to death was 3 days (IQR 1-6), and median length of stay was 6 days (IQR 1-12). SIRS criteria, the AVPU score, and the LODS had low positive (17-27.1, 33.3-43.9, 18.3-55.6%, respectively) and high negative predictive values (88.6-89.8, 86.5-91.2, 86.8-90.5%, respectively) for in-hospital mortality.
This pediatric sepsis cohort had high and early in-hospital mortality. Current criteria and tested clinical scores were inadequate for risk-stratification and mortality prediction in this population and setting. Pediatric sepsis management must take into account the local patient population, etiologies of sepsis, healthcare system, and resource availability. Only through studies such as this that generate regional data in LMICs can accurate risk stratification tools and context-appropriate, evidence-based guidelines be developed.
儿童脓毒症在全球范围内导致了相当高的发病率和死亡率,低收入和中等收入国家(LMICs)承担了大部分负担。由于资源限制和人群差异,国际脓毒症指南可能不适用于LMICs,尤其是撒哈拉以南非洲(SSA)地区。目前严重缺乏来自SSA地区的儿童脓毒症数据,没有这些数据就无法开发出准确的风险分层工具以及适合当地情况的循证方案。本研究的目的是描述坦桑尼亚一家公共急诊科(EMD)中儿童脓毒症的临床表现、干预措施及预后情况。
对2016年7月1日至9月30日期间在坦桑尼亚达累斯萨拉姆一家三级EMD就诊的脓毒症患儿(年龄28天至14岁,疑似感染且符合≥2条临床全身炎症反应综合征(SIRS)标准)进行前瞻性描述性研究。观察指标包括:住院死亡率(主要指标)、EMD死亡率和住院时间。我们使用均值和标准差、中位数和四分位数间距以及计数和百分比等方式报告描述性统计结果。对SIRS标准、清醒-言语-疼痛-无反应(AVPU)评分和兰巴雷内器官功能障碍评分(LODS)对住院、早期和晚期死亡率的预测能力进行了测试。
在筛查的2232名儿童中,433名(19.4%)符合纳入标准,405名被纳入研究。其中247名(61%)受试者是从外部机构转诊而来。约一半(54.1%)的受试者在EMD接受了抗生素治疗,35.8%(n = 145)的受试者进行了某种形式的微生物培养。住院死亡率和EMD死亡率分别为14.2%和1.5%,中位死亡时间为3天(四分位数间距1 - 6天),中位住院时间为6天(四分位数间距1 - 12天)。SIRS标准、AVPU评分和LODS对住院死亡率的阳性预测值较低(分别为17 - 27.1%、33.3 - 43.9%、18.3 - 55.6%),阴性预测值较高(分别为88.6 - 89.8%、86.5 - 91.2%、86.8 - 90.5%)。
该儿童脓毒症队列的住院死亡率高且出现较早。目前的标准和测试的临床评分在该人群和环境中不足以进行风险分层和死亡率预测。儿童脓毒症的管理必须考虑当地患者人群、脓毒症病因、医疗系统和资源可用性。只有通过此类在LMICs地区生成区域数据的研究,才能开发出准确的风险分层工具以及适合当地情况的循证指南。