Pujades-Rodriguez Mar, Guttmann Oliver P, Gonzalez-Izquierdo Arturo, Duyx Bram, O'Mahony Constantinos, Elliott Perry, Hemingway Harry
Leeds Institute of Biomedical and Clinical Sciences, University of Leeds, Leeds, United Kingdom.
Farr Institute of Health Informatics Research, Institute of Health Informatics, University College London, London, United Kingdom.
PLoS One. 2018 Jan 11;13(1):e0191214. doi: 10.1371/journal.pone.0191214. eCollection 2018.
To evaluate unmet clinical need in unselected hypertrophic cardiomyopathy (HCM) patients to determine the risk of a wide range of subsequent cardiovascular disease endpoints and safety endpoints relevant for trial design.
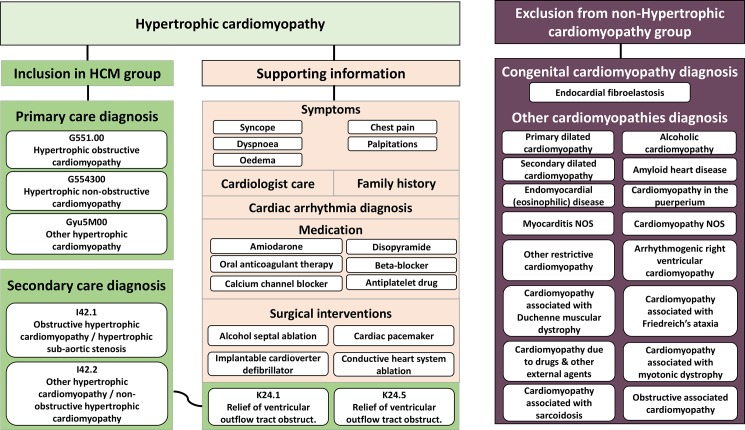
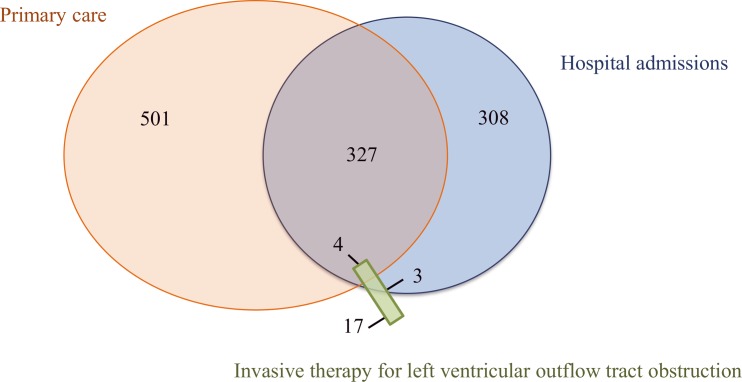
Population based cohort (CALIBER, linked primary care, hospital and mortality records in England, period 1997-2010), all people diagnosed with HCM were identified and matched by age, sex and general practice with ten randomly selected people without HCM. Random-effects Poisson models were used to assess the associations between HCM and cardiovascular diseases and bleeding.
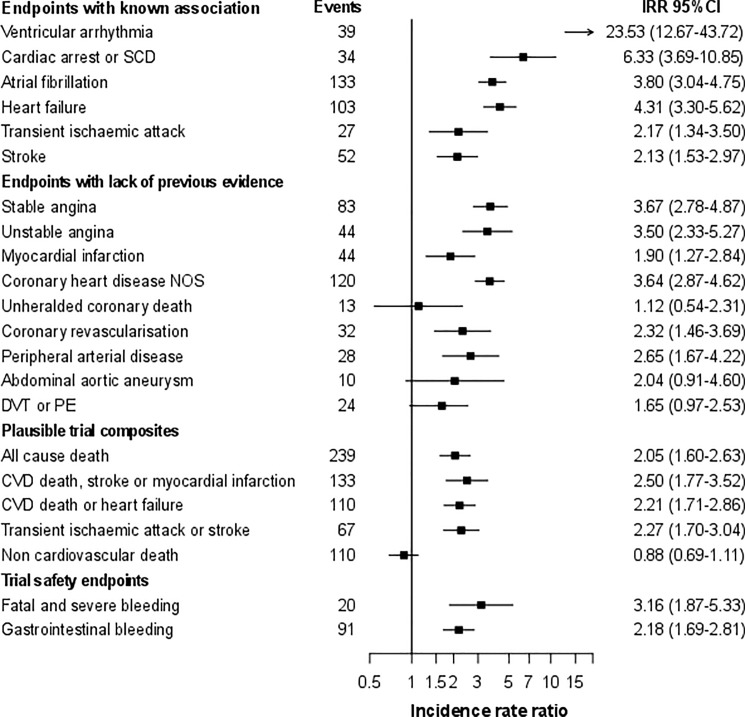
Among 3,290,455 eligible people a diagnosis of hypertrophic cardiomyopathy was found in 4 per 10,000. Forty-one percent of the 1,160 individuals with hypertrophic cardiomyopathy were women and the median age was 57 years. The median follow-up was 4.0 years. Compared to general population controls, people with HCM had higher risk of ventricular arrhythmia (incidence rate ratio = 23.53, [95% confidence interval 12.67-43.72]), cardiac arrest or sudden cardiac death (6.33 [3.69-10.85]), heart failure (4.31, [3.30-5.62]), and atrial fibrillation (3.80 [3.04-4.75]). HCM was also associated with a higher incidence of myocardial infarction ([MI] 1.90 [1.27-2.84]) and coronary revascularisation (2.32 [1.46-3.69]).The absolute Kaplan-Meier risks at 3 years were 8.8% for the composite endpoint of cardiovascular death or heart failure, 8.4% for the composite of cardiovascular death, stroke or myocardial infarction, and 1.5% for major bleeding.
Our study identified major unmet need in HCM and highlighted the importance of implementing improved cardiovascular prevention strategies to increase life-expectancy of the contemporary HCM population. They also show that national electronic health records provide an effective method for identifying outcomes and clinically relevant estimates of composite efficacy and safety endpoints essential for trial design in rare diseases.
评估未经选择的肥厚型心肌病(HCM)患者未满足的临床需求,以确定一系列后续心血管疾病终点事件和与试验设计相关的安全性终点事件的风险。
基于人群的队列研究(CALIBER,链接了英格兰1997 - 2010年期间的初级医疗、医院和死亡率记录),识别出所有诊断为HCM的患者,并按年龄、性别和全科医疗情况与随机选择的10名无HCM的患者进行匹配。采用随机效应泊松模型评估HCM与心血管疾病及出血之间的关联。
在3,290,455名符合条件的人群中,每10,000人中有4人被诊断为肥厚型心肌病。1,160例肥厚型心肌病患者中41%为女性,中位年龄为57岁。中位随访时间为4.0年。与普通人群对照组相比,HCM患者发生室性心律失常的风险更高(发病率比 = 23.53,[95%置信区间12.67 - 43.72])、心脏骤停或心源性猝死的风险更高(6.33 [3.69 - 10.85])、心力衰竭的风险更高(4.31,[3.30 - 5.62])以及心房颤动的风险更高(3.80 [3.04 - 4.75])。HCM还与心肌梗死([MI] 1.90 [1.27 - 2.84])和冠状动脉血运重建(2.32 [1.46 - 3.69])的较高发病率相关。3年时心血管死亡或心力衰竭复合终点事件的绝对Kaplan - Meier风险为8.8%,心血管死亡、卒中或心肌梗死复合终点事件的风险为8.4%,大出血的风险为1.5%。
我们的研究确定了HCM中主要未满足的需求,并强调了实施改进的心血管预防策略以提高当代HCM人群预期寿命的重要性。研究还表明,国家电子健康记录为识别结局以及对罕见病试验设计至关重要的复合疗效和安全性终点事件的临床相关估计提供了一种有效方法。