Johns Hopkins Hypertrophic Cardiomyopathy Center of Excellence, Baltimore, MD.
Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan.
J Am Heart Assoc. 2018 Feb 25;7(5):e006657. doi: 10.1161/JAHA.117.006657.
Hypertrophic cardiomyopathy (HCM) is a common inherited cardiac disease characterized by varying degrees of left ventricular outflow tract obstruction. In a large cohort, we compare the outcomes among 3 different hemodynamic groups.
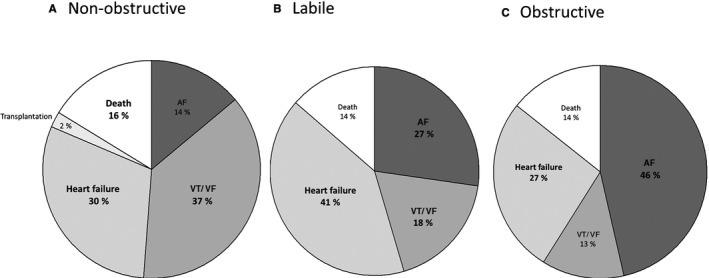
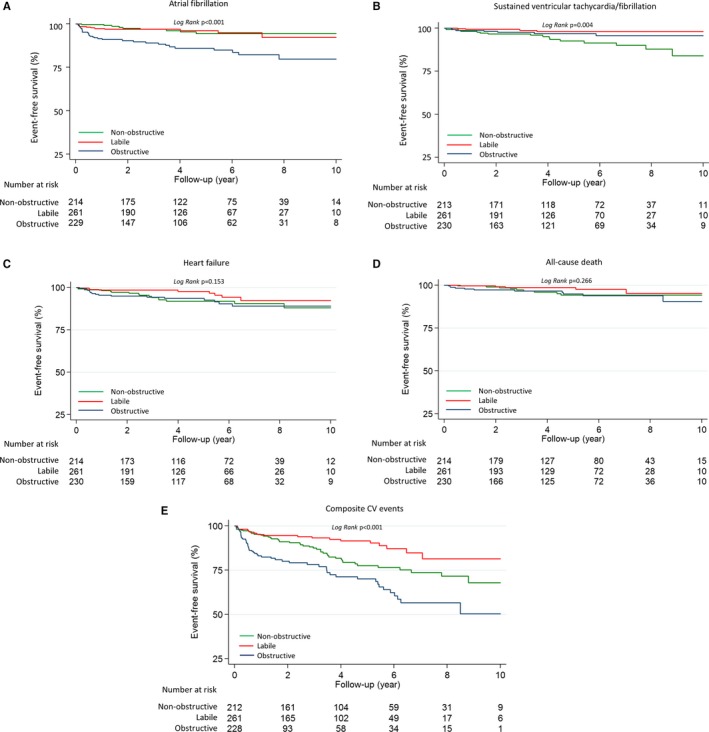
We prospectively enrolled patients fulfilling standard diagnostic criteria for HCM from January 2005 to June 2015. Detailed phenotypic characterization, including peak left ventricular outflow tract pressure gradients at rest and after provocation, was measured by echocardiography. The primary outcome was a composite cardiovascular end point, which included new-onset atrial fibrillation, new sustained ventricular tachycardia/ventricular fibrillation, new or worsening heart failure, and death. The mean follow-up was 3.4±2.8 years. Among the 705 patients with HCM (mean age, 52±15 years; 62% men), 230 with obstructive HCM were older and had a higher body mass index and New York Heart Association class. The 214 patients with nonobstructive HCM were more likely to have a history of sustained ventricular tachycardia/ventricular fibrillation and implantable cardioverter defibrillator implantation. During follow-up, 121 patients experienced a composite cardiovascular end point. Atrial fibrillation occurred most frequently in the obstructive group. Patients with nonobstructive HCM had more frequent sustained ventricular tachycardia/ventricular fibrillation events. In multivariate analysis, obstructive (hazard ratio, 2.80; 95% confidence interval, 1.64-4.80) and nonobstructive (hazard ratio, 1.94; 95% confidence interval, 1.09-3.45) HCM were associated with more adverse events compared with labile HCM.
Nonobstructive HCM carries notable morbidity, including a higher arrhythmic risk than the other HCM groups. Patients with labile HCM have a relatively benign clinical course. Our data suggest detailed sudden cardiac death risk stratification in nonobstructive HCM and monitoring with less aggressive management in labile HCM.
肥厚型心肌病(HCM)是一种常见的遗传性心脏病,其特征是左心室流出道梗阻程度不同。在一个大型队列中,我们比较了 3 个不同血流动力学组的结果。
我们前瞻性地招募了 2005 年 1 月至 2015 年 6 月符合 HCM 标准诊断标准的患者。通过超声心动图测量详细的表型特征,包括静息和激发后左心室流出道压力梯度的峰值。主要终点是心血管复合终点,包括新发心房颤动、新发持续性室性心动过速/心室颤动、新发或恶化心力衰竭和死亡。平均随访时间为 3.4±2.8 年。在 705 例 HCM 患者(平均年龄 52±15 岁,62%为男性)中,230 例梗阻性 HCM 患者年龄较大,体重指数和纽约心脏协会(NYHA)心功能分级较高。214 例非梗阻性 HCM 患者更有可能有持续性室性心动过速/心室颤动和植入式心脏复律除颤器植入的病史。随访期间,121 例患者发生心血管复合终点。梗阻性组心房颤动最常见。非梗阻性 HCM 患者持续性室性心动过速/心室颤动事件更频繁。多变量分析显示,梗阻性(危险比 2.80;95%置信区间 1.64-4.80)和非梗阻性(危险比 1.94;95%置信区间 1.09-3.45)HCM 与更多不良事件相关,而非波动性 HCM。
非梗阻性 HCM 发病率高,包括比其他 HCM 组更高的心律失常风险。波动性 HCM 患者的临床病程相对良性。我们的数据表明,非梗阻性 HCM 需要进行详细的猝死风险分层,并在波动性 HCM 中进行监测,采用不那么激进的管理策略。