Sun Ibrahim, Pamir M Necmettin
Neurosurgery, Acıbadem University, Istanbul, Turkey.
Front Neurol. 2017 Dec 20;8:672. doi: 10.3389/fneur.2017.00672. eCollection 2017.
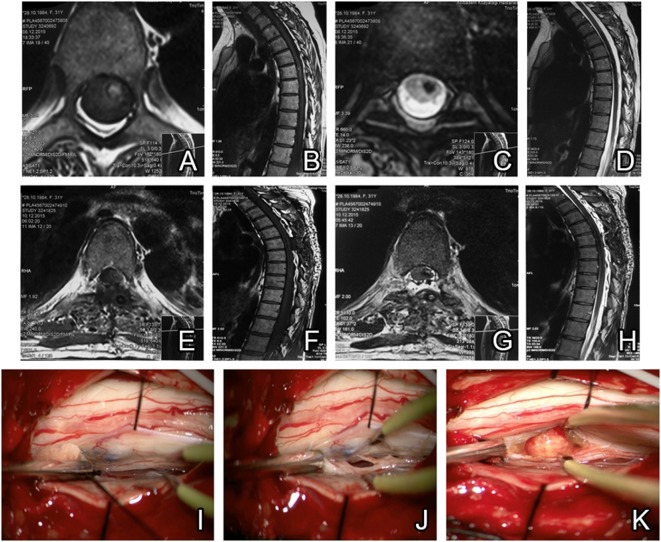
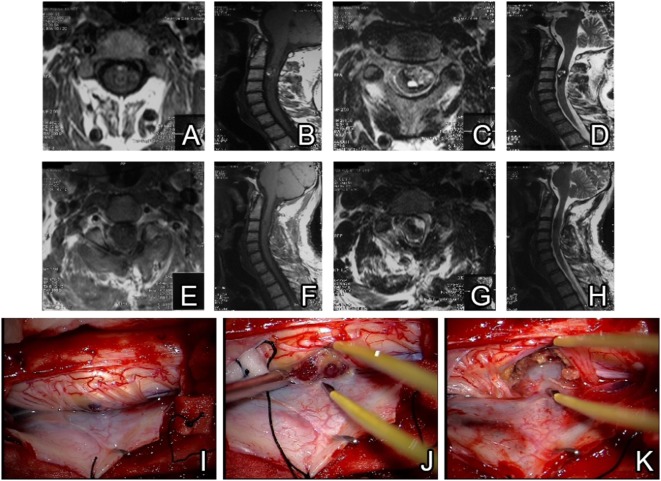
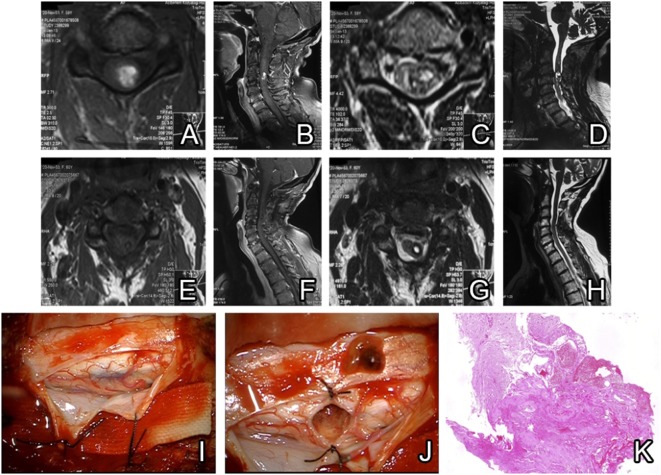
We report the preoperative and postoperative findings and also neurological follow-up results from 10 spinal cavernoma patients treated in our clinic. Several representative cases are presented in terms of clinical features, imaging results, and surgical outcomes.
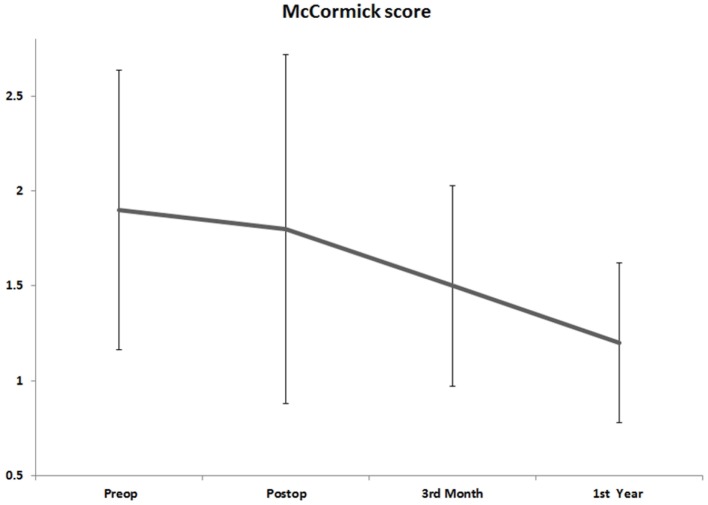
The data were retrospectively collected from patients' files in the hospital records and sorted with regards to clinical presentation, radiologic features, and operative findings. Patients received spinal MRI scans for the diagnosis of spinal cavernomas (SC) and postsurgical evaluation. Clinical presentation was evaluated Ogilvy classification and symptoms were checked preoperatively and postoperatively at third month and first year using McCormick scale. Primary treatment was microsurgical operation aiming a gross total lesion resection.
10 spinal cavernoma patients between the ages 30 and 63 were treated. Six (60%) of the patients were diagnosed with cervical and four (40%) others were diagnosed with thoracic SC. Among the patient group, mean preoperative Ogilvy classification score was 2.3 ± 0.7.8 and McCormick score was 1.9 ± 0.7. There was no residual mass or relapse after surgery. One patient developed surgery-related left hemiparesis, which was normalized at 1 year follow-up.
Patients must be diagnosed with MRI since it is nowadays a gold standard. Preoperative and postoperative scores are important in evaluating the patients' condition and improvement. The results from our patient series also reinforce the notion that immediate surgery should be the preferred treatment method for cavernomas. Intraoperative neurophysiologic monitarization should assist the surgery in order to prevent complications. In conclusion, microsurgery is a gold standard method that we recommend for cases of cavernomas, which will not recur if gross total resection is achieved.
我们报告了在我们诊所接受治疗的10例脊髓海绵状血管瘤患者的术前和术后检查结果以及神经学随访结果。从临床特征、影像学结果和手术结果方面展示了几个具有代表性的病例。
回顾性收集医院记录中患者档案的数据,并根据临床表现、放射学特征和手术所见进行分类。患者接受脊髓磁共振成像(MRI)扫描以诊断脊髓海绵状血管瘤(SC)并进行术后评估。根据奥吉尔维(Ogilvy)分类评估临床表现,并在术前以及术后第三个月和第一年使用麦科米克(McCormick)量表检查症状。主要治疗方法是显微手术,目标是实现肿瘤全切除。
治疗了10例年龄在30至63岁之间的脊髓海绵状血管瘤患者。其中6例(60%)患者被诊断为颈椎SC,另外4例(40%)被诊断为胸椎SC。在患者组中,术前奥吉尔维分类评分的平均值为2.3±0.78,麦科米克评分的平均值为1.9±0.7。术后无残留肿块或复发。1例患者出现了与手术相关的左侧偏瘫,在1年随访时恢复正常。
由于MRI如今是金标准,因此必须用其对患者进行诊断。术前和术后评分对于评估患者状况和病情改善很重要。我们患者系列的结果也强化了这样一种观念,即对于海绵状血管瘤,立即手术应是首选的治疗方法。术中神经生理监测应辅助手术以预防并发症。总之,显微手术是我们推荐用于海绵状血管瘤病例的金标准方法,如果实现肿瘤全切除则不会复发。