Department of Cardiovascular Ultrasound, The First Hospital of China Medical University, Shenyang, Liaoning, People's Republic of China, 110001.
Department of Cardiology, Mayo Clinic (Arizona), Scottsdale, Arizona, United States, 85259.
Int J Med Sci. 2018 Jan 1;15(2):108-114. doi: 10.7150/ijms.21956. eCollection 2018.
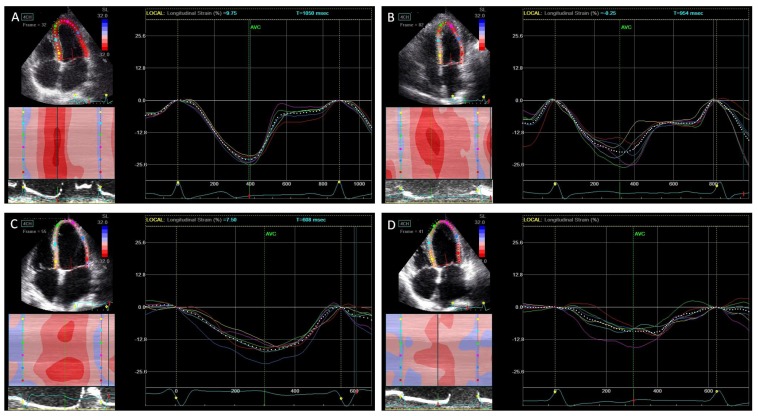
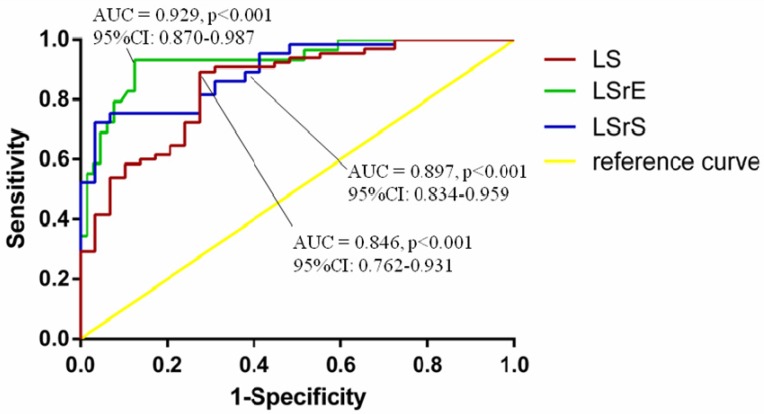
Mechanical dyssynchrony has been reported in heart failure with preserved ejection fraction (HFpEF), with a majority of patients having a narrow QRS complex; however, whether any benefit is observed with restoration of dyssynchrony remains unclear. We sought to assess left ventricular (LV) dyssynchrony and function in HFpEF and elucidate the underlying mechanisms that may account for HFpEF. Seventy-eighty patients with a narrow QRS complex including 47 with HFpEF, 31 with heart failure with reduced ejection fraction (HFrEF) patients, and 29 with asymptomatic left ventricular diastolic dysfunction (LVDD) were recruited. Forty-five normal subjects acted as controls. Systolic LV longitudinal strain (LS), systolic longitudinal strain rate (LSrS), early diastolic longitudinal strain rate (LSrE), and late diastolic longitudinal strain rate (LSrA) were measured using speckle tracking echocardiography. LV diastolic and systolic dyssynchrony (Te-SD and Ts-SD) were calculated. Te-SD and Ts-SD were prolonged in HFpEF and HFrEF patients than in the control group (<0.05). However, Ts-SD was shorter in HFpEF patients compared to HFrEF patients despite a narrow QRS complex (<0.05). LV global LS, LSrS, and LSrE were decreased in patients with HFpEF and HFrEF compared to other groups, with HFrEF being even more reduced than HFpEF (<0.05). Reduced LS, LSrS, and LSrE could effectively differentiate HF from asymptomatic LVDD patients (<0.05). HFrEF exhibited increased systolic dyssynchrony compared to HFpEF despite a narrow QRS complex in addition to the more reduced diastolic and systolic function. Therefore, targeting to improve diastolic and systolic function instead of managing systolic dyssynchrony might be of great importance in the treatment of HFpEF.
机械不同步已在射血分数保留的心力衰竭(HFpEF)患者中报告,其中大多数患者 QRS 波群较窄;然而,恢复不同步是否有任何益处尚不清楚。我们旨在评估 HFpEF 中的左心室(LV)不同步和功能,并阐明可能导致 HFpEF 的潜在机制。 我们招募了 78 名 QRS 波群较窄的患者,其中 47 名患有 HFpEF、31 名患有射血分数降低的心力衰竭(HFrEF)患者和 29 名无症状左心室舒张功能障碍(LVDD)患者。45 名正常受试者作为对照组。使用斑点追踪超声心动图测量收缩期 LV 纵向应变(LS)、收缩期纵向应变率(LSrS)、早期舒张期纵向应变率(LSrE)和晚期舒张期纵向应变率(LSrA)。计算 LV 舒张和收缩不同步(Te-SD 和 Ts-SD)。 HFpEF 和 HFrEF 患者的 Te-SD 和 Ts-SD 长于对照组(<0.05)。然而,尽管 QRS 波群较窄,但 HFpEF 患者的 Ts-SD 短于 HFrEF 患者(<0.05)。HFpEF 和 HFrEF 患者的 LV 整体 LS、LSrS 和 LSrE 低于其他组,HFrEF 比 HFpEF 降低更明显(<0.05)。降低的 LS、LSrS 和 LSrE 可以有效地将 HF 与无症状 LVDD 患者区分开(<0.05)。 尽管 QRS 波群较窄,但 HFrEF 与 HFpEF 相比,收缩不同步增加,舒张和收缩功能更降低。因此,针对改善舒张和收缩功能而不是管理收缩不同步可能在 HFpEF 的治疗中非常重要。