Osiyemi Olayemi, Yasin Salih, Zorrilla Carmen, Bicer Ceyhun, Hillewaert Vera, Brown Kimberley, Crauwels Herta M
Triple O Research Institute PA, West Palm Beach, FL, USA.
University of Miami School of Medicine, Miami, FL, USA.
Infect Dis Ther. 2018 Mar;7(1):147-159. doi: 10.1007/s40121-017-0184-8. Epub 2018 Jan 15.
Physiologic changes during pregnancy may impact the pharmacokinetics of drugs. In addition, efficacy and safety/tolerability concerns have been identified for some antiretroviral agents.
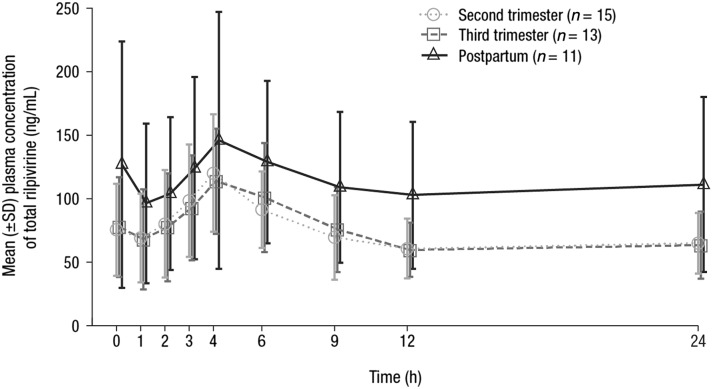
Human immunodeficiency virus (HIV)-1-infected pregnant women (18-26 weeks gestation) receiving the non-nucleoside reverse transcriptase inhibitor rilpivirine 25 mg once daily were enrolled in this phase 3b, open-label study examining the impact of pregnancy on the pharmacokinetics of rilpivirine when it is given in combination with other antiretroviral agents. Blood samples (collected over the 24-h dosing interval) to assess total and unbound rilpivirine plasma concentrations were obtained during the second and third trimesters (24-28 and 34-38 weeks gestation, respectively) and 6-12 weeks postpartum. Pharmacokinetic parameters were derived using noncompartmental analysis and compared (pregnancy versus postpartum) using linear mixed effects modeling. Antiviral and immunologic response and safety were assessed.
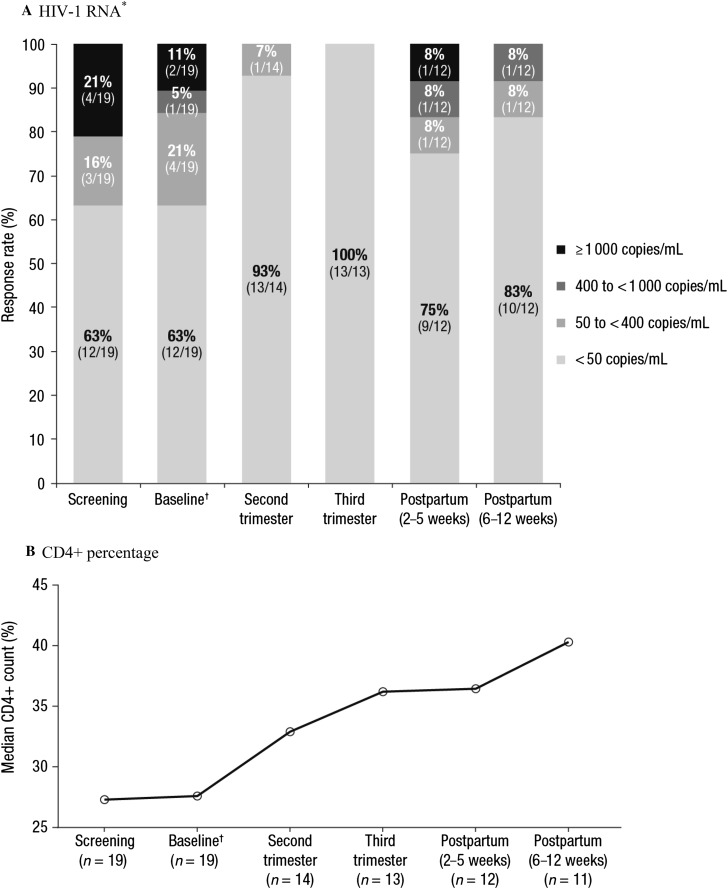
Nineteen women were enrolled; 15 had evaluable pharmacokinetic results. Total rilpivirine exposure was 29-31% lower during pregnancy versus postpartum; differences were less pronounced for unbound (pharmacodynamically active) rilpivirine. At study entry, 12/19 (63.2%) women were virologically suppressed; 10/12 (83.3%) women were suppressed at the postpartum visit. Twelve infants were born to the 12 women who completed the study (7 discontinued); no perinatal viral transmission was observed among 10 infants with available data. Rilpivirine was generally safe and well tolerated in women and infants exposed in utero.
Despite decreased rilpivirine exposure during pregnancy, treatment was effective in preventing mother-to-child transmission and suppressing HIV-1 RNA in pregnant women. Results suggest that rilpivirine 25 mg once daily, as part of individualized combination antiretroviral therapy, may be an appropriate option for HIV-1-infected pregnant women.
ClinicalTrials.gov Identifier, NCT00855335.
孕期的生理变化可能会影响药物的药代动力学。此外,一些抗逆转录病毒药物的疗效及安全性/耐受性也受到关注。
本3b期开放标签研究纳入了感染人类免疫缺陷病毒1型(HIV-1)、妊娠18 - 26周且每日一次接受25mg非核苷类逆转录酶抑制剂利匹韦林治疗的孕妇,旨在研究孕期与其他抗逆转录病毒药物联用时对利匹韦林药代动力学的影响。在孕中期和孕晚期(分别为妊娠24 - 28周和34 - 38周)以及产后6 - 12周采集血样(在24小时给药间隔内收集),以评估利匹韦林的总血浆浓度和游离血浆浓度。采用非房室分析法得出药代动力学参数,并使用线性混合效应模型进行比较(孕期与产后)。评估抗病毒和免疫反应以及安全性。
共纳入19名女性;15名有可评估的药代动力学结果。孕期利匹韦林的总暴露量比产后低29% - 31%;游离(具有药效学活性)利匹韦林的差异则不那么明显。研究开始时,12/19(63.2%)的女性病毒得到抑制;产后访视时,10/12(83.3%)的女性病毒得到抑制。完成研究的12名女性共分娩12名婴儿(7名中断治疗);在有可用数据的10名婴儿中未观察到围产期病毒传播。利匹韦林对子宫内暴露的女性和婴儿总体安全且耐受性良好。
尽管孕期利匹韦林暴露量降低,但治疗在预防母婴传播和抑制孕妇HIV-1 RNA方面有效。结果表明,作为个体化联合抗逆转录病毒治疗的一部分,每日一次25mg利匹韦林可能是HIV-1感染孕妇的合适选择。
ClinicalTrials.gov标识符,NCT00855335。