Alsolamy Sami, Al-Sabhan Atheer, Alassim Najla, Sadat Musharaf, Qasim Eman Al, Tamim Hani, Arabi Yaseen M
Emergency Medicine and Intensive Care Department, College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, King Abdulaziz Medical City, Riyadh, Kingdom of Saudi Arabia.
Emergency Medicine Department, King Abdulaziz Medical City, Riyadh, Kingdom of Saudi Arabia.
BMC Emerg Med. 2018 Jan 18;18(1):3. doi: 10.1186/s12873-018-0155-8.
Clinical handover is an important process for the transition of patient-care responsibility to the next healthcare provider, but it may divert the attention of the team away from active patients. This is challenging in the Emergency Department (ED) because of highly dynamic patient conditions and is likely relevant in conditions that requires time-sensitive therapies, such as sepsis. We aimed to examine the management and outcomes of patients presenting with sepsis and septic shock to the ED during nursing handover.
This retrospective cohort study was conducted at a 115-bed ED and more than 200,000 annual ED visits, within a 900-bed academic tertiary care center. Data on Surviving Sepsis Campaign (SSC) bundle elements and hospital mortality were collected for all ≥14-year-old patients who presented to the ED with a diagnosis of sepsis and septic shock between January 1, 2011 and October 30, 2013. Our primary outcome was time to antibiotics, were other SSC bundle elements and mortality counted as secondary outcomes. Patients were divided into two groups: 1) handover time group, comprising patients who presented an hour before or after the start of handover time (6-8 AM/PM), and 2) non-handover time group, comprising patients who presented over the remaining 20 h.
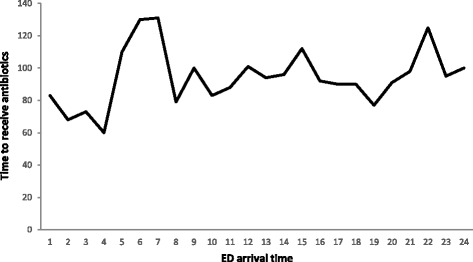
During the study period, 1330 patients presented with sepsis or septic shock (228, handover time group; 1102, non-handover time group). No significant differences were found between the handover time and non-handover time groups, respectively, in median time to antibiotic administration (100 [interquartile range (IQR) 57-172] vs. 95 [IQR 50-190] minutes; P = 0.07), median time to serum lactate result (162 [IQR 108-246] vs. 156 [IQR 180-246] minutes; P = 0.33) and median time to obtain blood culture (54 [IQR 36-119] vs. 52 [IQR 28-103] minutes; P = 0.52), and hospital mortality rate (29.4% vs. 28.9%; P = 0.89).
No significant differences were found in median time of SSC bundle elements or hospital mortality between patients who presented during the handover and non-handover times.
临床交接班是将患者护理责任移交给下一位医疗服务提供者的重要过程,但它可能会使团队的注意力从正在接受治疗的患者身上转移开。在急诊科(ED),由于患者病情高度动态变化,这一情况颇具挑战性,并且在需要及时治疗的病症(如脓毒症)中可能也存在类似问题。我们旨在研究在护理交接班期间急诊科收治的脓毒症和脓毒性休克患者的管理及预后情况。
这项回顾性队列研究在一家拥有115张床位的急诊科进行,该急诊科每年接待超过200,000名患者,隶属于一家拥有900张床位的学术型三级医疗中心。收集了2011年1月1日至2013年10月30日期间所有年龄≥14岁、因脓毒症和脓毒性休克诊断而就诊于急诊科的患者的“拯救脓毒症运动”(SSC)集束化治疗要素及医院死亡率数据。我们的主要结局指标是给予抗生素的时间,其他SSC集束化治疗要素及死亡率作为次要结局指标。患者被分为两组:1)交接班时间组,包括在交接班时间(上午/下午6 - 8点)开始前或后一小时内就诊的患者;2)非交接班时间组,包括在其余20小时内就诊的患者。
在研究期间,1330例患者被诊断为脓毒症或脓毒性休克(228例在交接班时间组;1102例在非交接班时间组)。交接班时间组和非交接班时间组在给予抗生素的中位时间(100[四分位间距(IQR)57 - 172]分钟 vs. 95[IQR 50 - 190]分钟;P = 0.07)、血清乳酸检测结果的中位时间(162[IQR 108 - 246]分钟 vs. 156[IQR 180 - 246]分钟;P = 0.33)、获取血培养的中位时间(54[IQR 36 - 119]分钟 vs. 52[IQR 28 - 103]分钟;P = 0.52)以及医院死亡率(29.4% vs. 28.9%;P = 0.89)方面均未发现显著差异。
在交接班时间就诊和非交接班时间就诊的患者之间,SSC集束化治疗要素的中位时间或医院死亡率未发现显著差异。