Health Economics at Bristol, Population Health Sciences, Bristol Medical School, University of Bristol, Bristol, BS8 2PS, UK.
Collaboration for Leadership in Applied Health Research and Care West at University Hospitals Bristol, Bristol, BS1 2NT, UK.
BMC Cancer. 2018 Jan 18;18(1):84. doi: 10.1186/s12885-017-3974-1.
There is ongoing debate about the harms and benefits of a national prostate cancer screening programme. Several model-based cost-effectiveness analyses have been developed to determine whether the benefits of prostate cancer screening outweigh the costs and harms caused by over-detection and over-treatment, and the different approaches may impact results.
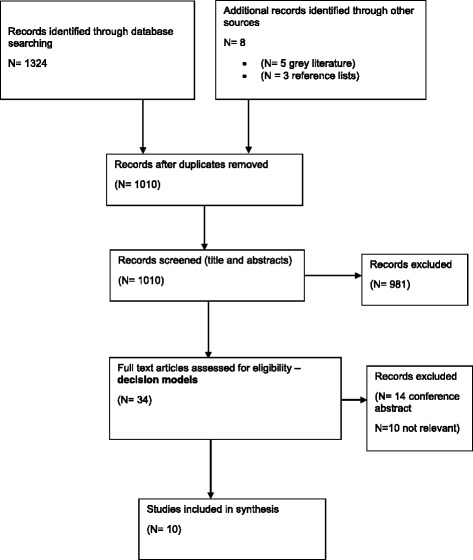
To identify models of prostate cancer used to assess the cost-effectiveness of prostate cancer screening strategies, a systematic review of articles published since 2006 was conducted using the NHS Economic Evaluation Database, Medline, EMBASE and HTA databases. The NICE website, UK National Screening website, reference lists from relevant studies were also searched and experts contacted. Key model features, inputs, and cost-effectiveness recommendations were extracted.
Ten studies were included. Four of the studies identified some screening strategies to be potentially cost-effective at a PSA threshold of 3.0 ng/ml, including single screen at 55 years, annual or two yearly screens starting at 55 years old, and delayed radical treatment. Prostate cancer screening was modelled using both individual and cohort level models. Model pathways to reflect cancer progression varied widely, Gleason grade was not always considered and clinical verification was rarely outlined. Where quality of life was considered, the methods used did not follow recommended practice and key issues of overdiagnosis and overtreatment were not addressed by all studies.
The cost-effectiveness of prostate cancer screening is unclear. There was no consensus on the optimal model type or approach to model prostate cancer progression. Due to limited data availability, individual patient-level modelling is unlikely to increase the accuracy of cost-effectiveness results compared with cohort-level modelling, but is more suitable when assessing adaptive screening strategies. Modelling prostate cancer is challenging and the justification for the data used and the approach to modelling natural disease progression was lacking. Country-specific data are required and recommended methods used to incorporate quality of life. Influence of data inputs on cost-effectiveness results need to be comprehensively assessed and the model structure and assumptions verified by clinical experts.
关于国家前列腺癌筛查计划的危害和益处,目前仍存在争议。已经开展了几项基于模型的成本效益分析,以确定前列腺癌筛查是否利大于弊,是否超过了过度检测和过度治疗所带来的成本和危害,而不同的方法可能会影响结果。
为了确定用于评估前列腺癌筛查策略成本效益的前列腺癌模型,我们使用 NHS 经济评估数据库、Medline、EMBASE 和 HTA 数据库,对 2006 年以来发表的文章进行了系统回顾。还检索了 NICE 网站、英国国家筛查网站、相关研究的参考文献列表,并联系了专家。提取了关键模型特征、输入和成本效益建议。
共纳入 10 项研究。其中 4 项研究确定了一些在 PSA 阈值为 3.0ng/ml 时具有潜在成本效益的筛查策略,包括 55 岁时单次筛查、55 岁开始每年或每两年筛查、延迟根治性治疗。前列腺癌筛查采用个体和队列水平模型进行建模。反映癌症进展的模型途径差异很大,未始终考虑 Gleason 分级,且很少概述临床验证。在考虑生活质量的地方,使用的方法不符合推荐做法,并非所有研究都解决了过度诊断和过度治疗的关键问题。
前列腺癌筛查的成本效益尚不清楚。对于最佳模型类型或建模前列腺癌进展的方法,尚未达成共识。由于数据有限,与队列水平建模相比,个体患者水平建模不太可能提高成本效益结果的准确性,但在评估适应性筛查策略时更合适。建模前列腺癌具有挑战性,缺乏对所用数据的合理性以及对自然疾病进展建模方法的论证。需要有特定国家的数据,并建议使用纳入生活质量的方法。需要全面评估数据输入对成本效益结果的影响,并由临床专家验证模型结构和假设。