Kim Paul, Lee Ju Kang, Lim Oh Kyung, Park Heung Kyu, Park Ki Deok
Department of Rehabilitation Medicine, Gachon University Gil Medical Center, Incheon, Korea.
Department of Breast Surgery, Gachon University Gil Medical Center, Incheon, Korea.
Ann Rehabil Med. 2017 Dec;41(6):1065-1075. doi: 10.5535/arm.2017.41.6.1065. Epub 2017 Dec 28.
To predict the probability of lymphedema development in breast cancer patients in the early post-operation stage, we investigated the ability of quantitative lymphoscintigraphic assessment.
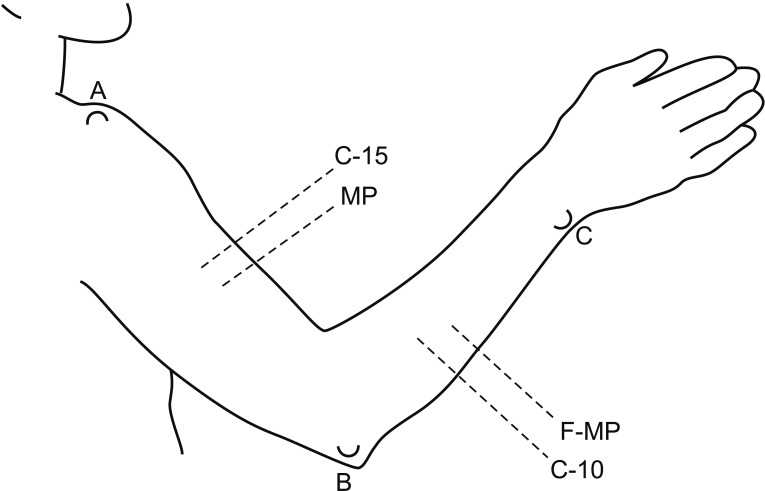
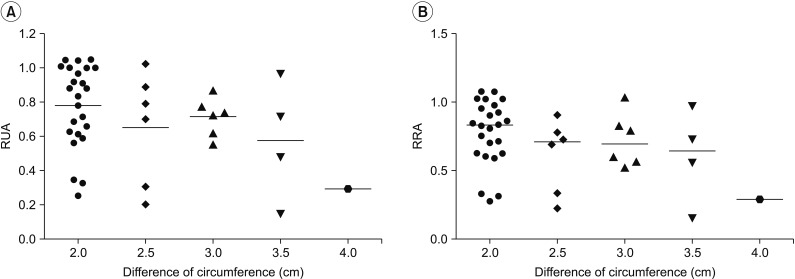
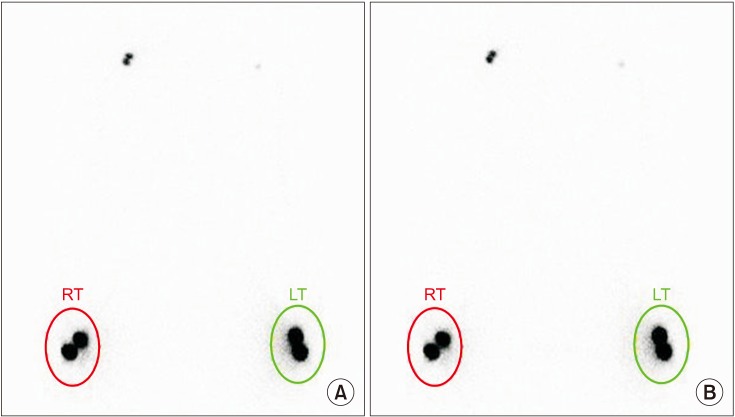
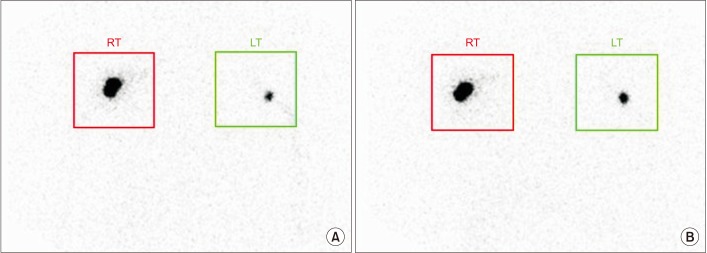
This retrospective study included 201 patients without lymphedema after unilateral breast cancer surgery. Lymphoscintigraphy was performed between 4 and 8 weeks after surgery to evaluate the lymphatic system in the early postoperative stage. Quantitative lymphoscintigraphy was performed using four methods: ratio of radiopharmaceutical clearance rate of the affected to normal hand; ratio of radioactivity of the affected to normal hand; ratio of radiopharmaceutical uptake rate of the affected to normal axilla (RUA); and ratio of radioactivity of the affected to normal axilla (RRA). During a 1-year follow-up, patients with a circumferential interlimb difference of 2 cm at any measurement location and a 200-mL interlimb volume difference were diagnosed with lymphedema. We investigated the difference in quantitative lymphoscintigraphic assessment between the non-lymphedema and lymphedema groups.
Quantitative lymphoscintigraphic assessment revealed that the RUA and RRA were significantly lower in the lymphedema group than in the non-lymphedema group. After adjusting the model for all significant variables (body mass index, N-stage, T-stage, type of surgery, and type of lymph node surgery), RRA was associated with lymphedema (odds ratio=0.14; 95% confidence interval, 0.04-0.46; p=0.001).
In patients in the early postoperative stage after unilateral breast cancer surgery, quantitative lymphoscintigraphic assessment can be used to predict the probability of developing lymphedema.
为预测乳腺癌患者术后早期发生淋巴水肿的概率,我们研究了定量淋巴闪烁显像评估的能力。
这项回顾性研究纳入了201例单侧乳腺癌手术后无淋巴水肿的患者。在术后4至8周进行淋巴闪烁显像,以评估术后早期的淋巴系统。采用四种方法进行定量淋巴闪烁显像:患侧与健侧手部放射性药物清除率之比;患侧与健侧手部放射性之比;患侧与健侧腋窝放射性药物摄取率之比(RUA);患侧与健侧腋窝放射性之比(RRA)。在1年的随访期间,任何测量部位肢体周径差值达2 cm且肢体体积差值达200 mL的患者被诊断为淋巴水肿。我们研究了非淋巴水肿组和淋巴水肿组在定量淋巴闪烁显像评估方面的差异。
定量淋巴闪烁显像评估显示,淋巴水肿组的RUA和RRA显著低于非淋巴水肿组。在对所有显著变量(体重指数、N分期、T分期、手术类型和淋巴结手术类型)进行模型调整后,RRA与淋巴水肿相关(比值比=0.14;95%置信区间,0.04 - 0.46;p = 0.001)。
在单侧乳腺癌手术后的早期患者中,定量淋巴闪烁显像评估可用于预测发生淋巴水肿的概率。