Ho Nhan Thi, Thompson Corinne, Nhan Le Nguyen Thanh, Van Hoang Minh Tu, Dung Nguyen Thanh, Tran My Phuc, Quang Vo Minh, Minh Ngo Ngoc Quang, Tuan Tran Anh, Hung Nguyen Thanh, Tuan Ha Manh, Vinh Chau Nguyen Van, Wolbers Marcel, Thwaites Guy E, Choisy Marc, Baker Stephen
Oxford University Clinical Research Unit, Wellcome Trust Major Overseas Program, Ho Chi Minh City, Vietnam.
Pediatrics, Columbia UniversityMedical Center, New York, New York, United States.
BMJ Open. 2018 Jan 21;8(1):e016349. doi: 10.1136/bmjopen-2017-016349.
Acute respiratory tract infections (ARIs) are the leading cause of morbidity and mortality in young children in low/middle-income countries. Using routine hospital data, we aimed to examine the spatial distribution, temporal trends and climatic risk factors of paediatric ARIs in Vietnam.
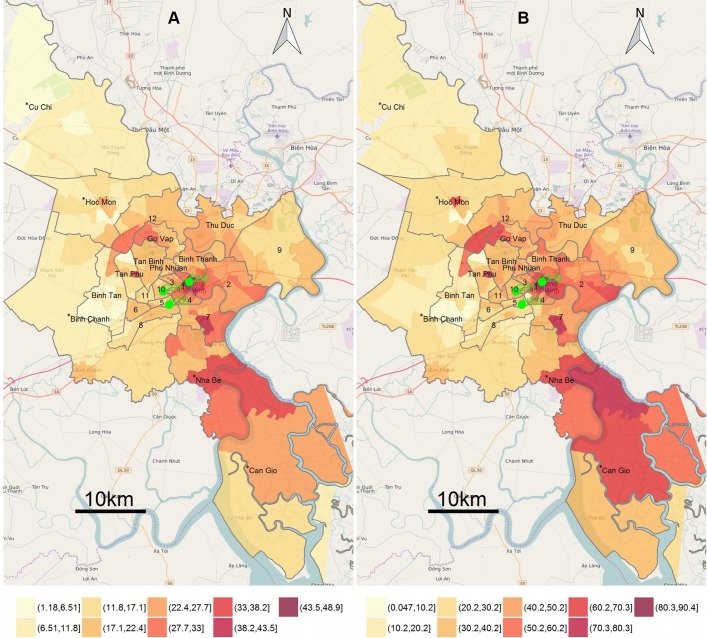
Data from hospitalised paediatric (<16 years) patients with ARIs residing in Ho Chi Minh City (HCMC) between 2005 and 2010 were retrieved from the two main Children's Hospitals and the Hospital for Tropical Diseases in HCMC. Spatial mapping and time series analysis were performed after disaggregating data into upper respiratory tract infections (URIs) and lower respiratory tract infections (LRIs).
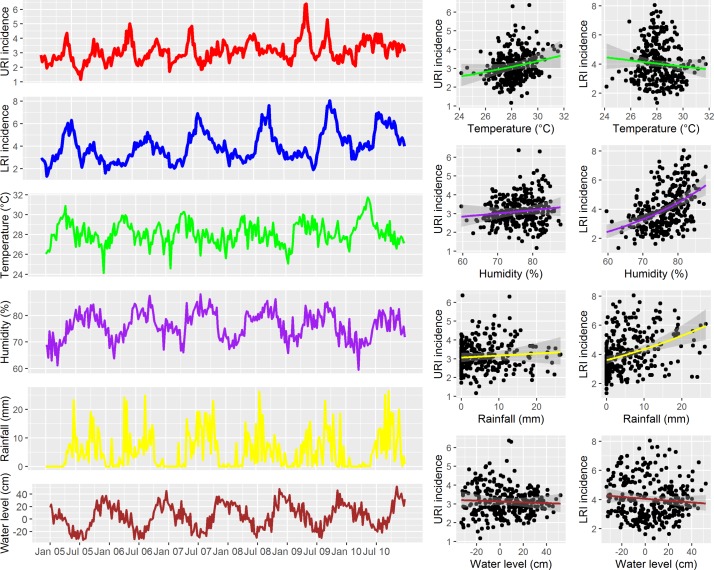
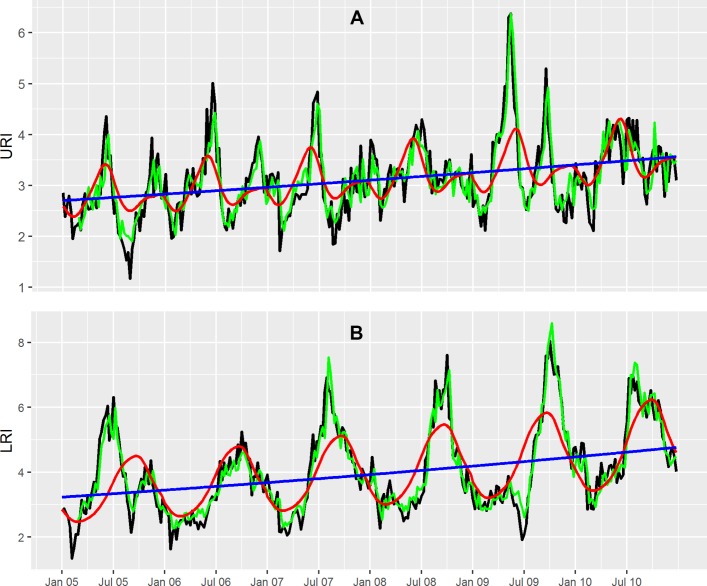
Over the study period, there were 155 999 paediatric patients admitted with ARIs (33% of all hospital admissions). There were 68 120 URIs (14%) and 87 879 LRIs (19%). The most common diagnoses were acute pharyngitis (28% of all ARI), pneumonia (21%), bronchitis (18%) and bronchiolitis (16%). A significant increasing trend over time was found for both URIs (mean weekly incidence per 1000 population, I=3.12), incidence rate ratio for 1-week increase in time (RR 1.0, 95% CI 1.02 to 1.17) for URI and (I=4.02, RR 1.08 (95% CI 1.006 to 1.16)) for LRI. The weekly URI incidence peaked in May-June and was significantly associated with lags in weekly URI incidence and the average humidity, rainfall and water level. The weekly LRI incidence exhibited significant seasonality (P<0.0001), with an annual peak in September-October and was significantly associated with lags in weekly LRI incidence and lags in weekly average temperature, rainfall and water level.
ARIs are a leading cause of childhood hospitalisation in HCMC, Vietnam. The incidence of ARIs was higher in the wet season and in specific HCMC districts. These results may guide health authorities in where and when to effectively allocate resources for the prevention and control of ARIs.
在低收入/中等收入国家,急性呼吸道感染(ARI)是幼儿发病和死亡的主要原因。我们旨在利用医院常规数据,研究越南儿童ARI的空间分布、时间趋势和气候风险因素。
从胡志明市(HCMC)两家主要儿童医院和热带病医院获取2005年至2010年期间住院的ARI儿科(<16岁)患者的数据。将数据分解为上呼吸道感染(URI)和下呼吸道感染(LRI)后,进行空间映射和时间序列分析。
在研究期间,有155999名儿科患者因ARI入院(占所有住院人数的33%)。其中有68120例URI(占14%)和87879例LRI(占19%)。最常见的诊断为急性咽炎(占所有ARI的28%)、肺炎(21%)、支气管炎(18%)和细支气管炎(16%)。发现URI(每1000人口每周平均发病率,I = 3.12)和LRI(I = 4.02)随时间均呈显著上升趋势,URI每增加1周的发病率比值比(RR 1.0,95%CI 1.02至1.17),LRI为RR 1.08(95%CI 1.006至1.16)。每周URI发病率在5月至6月达到峰值,且与每周URI发病率的滞后以及平均湿度、降雨量和水位显著相关。每周LRI发病率呈现出显著的季节性(P < 0.0001),在9月至10月达到年度峰值,且与每周LRI发病率的滞后以及每周平均温度、降雨量和水位的滞后显著相关。
在越南胡志明市,ARI是儿童住院的主要原因。ARI发病率在雨季和胡志明市的特定地区较高。这些结果可为卫生当局在何时何地有效分配资源以预防和控制ARI提供指导。