Meier Richard, Bi Chengpeng, Gaedigk Roger, Heruth Daniel P, Ye Shui Qing, Leeder J Steven, Fridley Brooke L
Department of Biostatistics, University of Kansas Medical Center.
Division of Clinical Pharmacology, Toxicology and Therapeutic Innovation.
Pharmacogenet Genomics. 2018 Mar;28(3):86-94. doi: 10.1097/FPC.0000000000000326.
The majority of drug dosing studies are based on adult populations, with modification of the dosing for children based on size and weight. This rudimentary approach for drug dosing children is limited, as biologically a child can differ from an adult in far more aspects than just size and weight. Specifically, understanding the ontogeny of childhood liver development is critical in dosing drugs that are metabolized through the liver, as the rate of metabolism determines the duration and intensity of a drug's pharmacologic action. Therefore, we set out to determine pharmacogenes that change over childhood development, followed by a secondary agnostic analysis, assessing changes transcriptome wide.
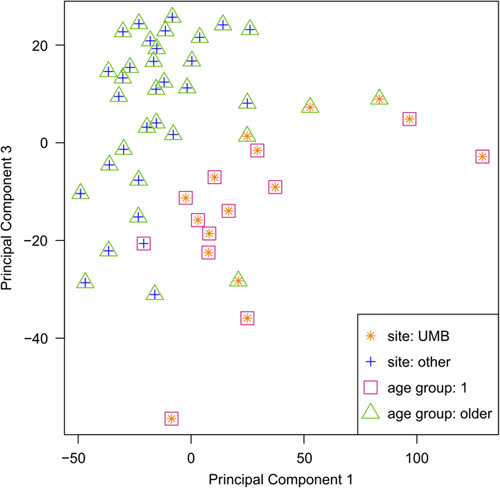
A total of 47 human liver tissue samples, with between 10 and 13 samples in four age groups spanning childhood development, underwent pair-end sequencing. Kruskal-Wallis and Spearman's rank correlation tests were used to determine the association of gene expression levels with age. Gene set analysis based on the pathways in KEGG utilized the gamma method. Correction for multiple testing was completed using q-values.
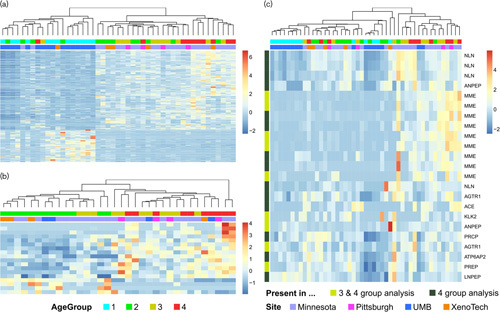
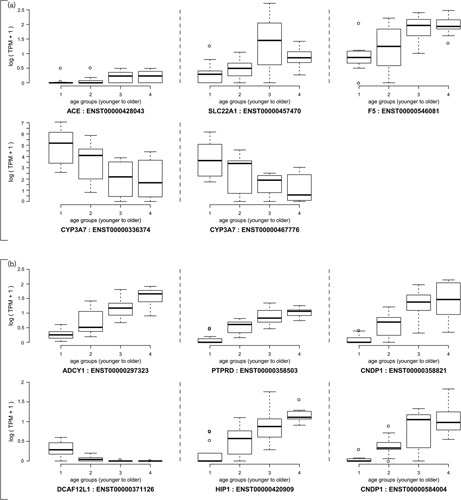
We found evidence for increased expression of 'very important pharmacogenes', for example, coagulation factor V (F5) (P=6.7×10(-7)), angiotensin I converting enzyme (ACE) (P=6.4×10(-3)), and solute carrier family 22 member 1 (SLC22A1) (P=7.0×10(-5)) over childhood development. In contrast, we observed a significant decrease in expression of two alternative CYP3A7 transcripts (P=1.5×10(-5) and 3.0×10(-5)) over development. The analysis of genome-wide changes detected transcripts in the following genes with significant changes in mRNA expression (P<1×10(-9) with false discovery rate<5×0(-5)): ADCY1, PTPRD, CNDP1, DCAF12L1 and HIP1. Gene set analysis determined ontogeny-related transcriptomic changes in the renin-angiotensin pathway (P<0.002), with lower expression of the pathway, in general, observed in liver samples from younger participants.
Considering that the renin-angiotensin pathway plays a central role in blood pressure and plasma sodium concentration, and our observation that ACE and PTPRD expression increased over the spectrum of childhood development, this finding could potentially impact the dosing of an entire class of drugs known as ACE-inhibitors in pediatric patients.
大多数药物剂量研究基于成年人群,儿童药物剂量根据体型和体重进行调整。这种给儿童用药的基本方法存在局限性,因为从生物学角度来看,儿童与成人的差异远不止体型和体重。具体而言,了解儿童肝脏发育的个体发生过程对于给通过肝脏代谢的药物给药至关重要,因为代谢速率决定了药物药理作用的持续时间和强度。因此,我们着手确定在儿童发育过程中发生变化的药物基因,随后进行二次无假设分析,评估全转录组范围的变化。
总共47份人类肝脏组织样本,在涵盖儿童发育的四个年龄组中每组有10至13个样本,进行了双末端测序。使用Kruskal-Wallis检验和Spearman秩相关检验来确定基因表达水平与年龄的关联。基于KEGG通路的基因集分析采用伽马方法。使用q值完成多重检验校正。
我们发现证据表明,在儿童发育过程中,“非常重要的药物基因”表达增加,例如凝血因子V(F5)(P = 6.7×10⁻⁷)、血管紧张素I转换酶(ACE)(P = 6.4×10⁻³)和溶质载体家族22成员1(SLC22A1)(P = 7.0×10⁻⁵)。相比之下,我们观察到两种CYP3A7可变转录本的表达在发育过程中显著下降(P = 1.5×10⁻⁵和3.0×10⁻⁵)。全基因组变化分析检测到以下基因的转录本mRNA表达有显著变化(错误发现率<5×10⁻⁵时P<1×10⁻⁹):ADCY1、PTPRD、CNDP1、DCAF12L1和HIP1。基因集分析确定了肾素 - 血管紧张素途径中与个体发生相关的转录组变化(P<0.002),总体而言,在较年轻参与者的肝脏样本中观察到该途径的表达较低。
鉴于肾素 - 血管紧张素途径在血压和血浆钠浓度中起核心作用,以及我们观察到ACE和PTPRD表达在儿童发育过程中增加,这一发现可能会影响儿科患者中一类称为ACE抑制剂的药物的剂量。