Devillers Louise, Sicsic Jonathan, Delbarre Angelique, Le Bel Josselin, Ferrat Emilie, Saint Lary Olivier
Department of Family Medicine, Faculty of Health Sciences Simone Veil, University Versailles Saint-Quentin en Yvelines (UVSQ), Montigny-le-Bretonneux, France.
CESP, University Paris-Sud, UVSQ, INSERM U1018, University Paris-Saclay, Villejuif, France.
PLoS One. 2018 Jan 25;13(1):e0190522. doi: 10.1371/journal.pone.0190522. eCollection 2018.
Antibiotic prescription is a central public health issue. Overall, 90% of antibiotic prescriptions are delivered to patients in ambulatory care, and a substantial proportion of these prescriptions could be avoided. General Practitioner (GP) trainers are similar to other GPs in terms of sociodemographic and medical activities, but they may have different prescription patterns. Our aim was to compare the antibiotic prescribing rates between GP trainers and non-trainers.
This observational cross-sectional study was conducted on administrative data claims from the French National Health Insurance. The antibiotic prescribing rate was calculated. The main independent variable was the training status of the GPs. Prescribing rates were adjusted for the various GPs' characteristics (gender, age, location of the practice, number of visits per GP and the case-mix) in a multiple linear regression analysis.
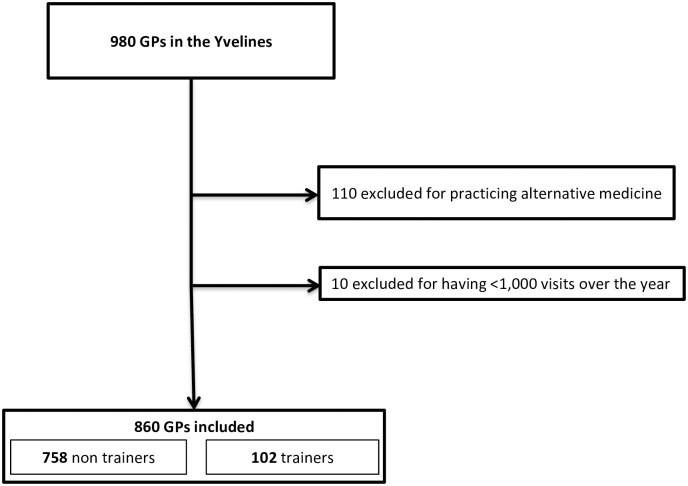
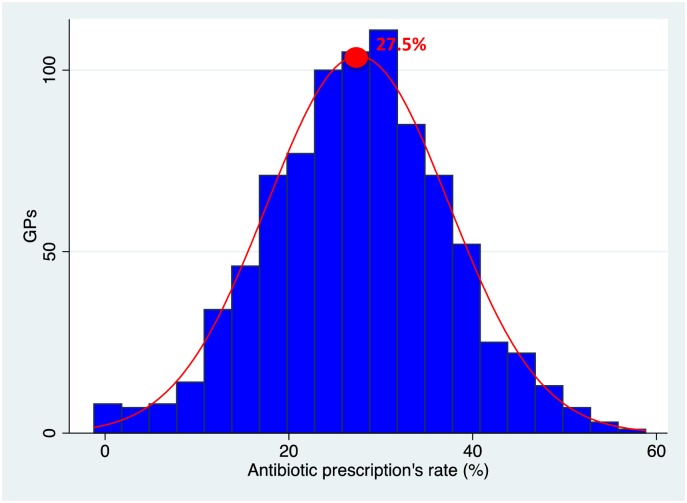
Between June 2014 and July 2015 the prescribing patterns of 860 GPs were analysed, among which 102 were GP trainers (12%). Over the year 363,580 patients were prescribed an antibiotic out of 3,499,248 visits for 1,299,308 patients seen over the year thus representing around 27.5% of patients. In the multivariate analyses, being a trainer resulted in a significant difference of 6.62 percentage points (IC 95%: [-8.55; -4.69]; p<0.001) in antibiotic prescriptions comparing to being a non-trainer, corresponding to a relative reduction of 23.4%.
These findings highlight the role of GP trainers in antibiotic prescriptions. By prescribing fewer antibiotics and influencing the next generations of GPs, the human and economic burden of antibiotics could be reduced.
抗生素处方是一个核心公共卫生问题。总体而言,90%的抗生素处方是开给门诊患者的,其中很大一部分处方是可以避免的。全科医生(GP)培训师在社会人口统计学和医疗活动方面与其他全科医生相似,但他们可能有不同的处方模式。我们的目的是比较全科医生培训师和非培训师之间的抗生素处方率。
本观察性横断面研究基于法国国家医疗保险的行政数据索赔进行。计算抗生素处方率。主要自变量是全科医生的培训状态。在多元线性回归分析中,根据全科医生的各种特征(性别、年龄、执业地点、每位全科医生的就诊次数和病例组合)对处方率进行调整。
在2014年6月至2015年7月期间,分析了860名全科医生的处方模式,其中102名是全科医生培训师(12%)。在这一年中,3499248次就诊的1299308名患者中有363580名患者被开了抗生素,因此约占患者的27.5%。在多变量分析中,与非培训师相比,作为培训师的抗生素处方率有6.62个百分点的显著差异(95%置信区间:[-8.55;-4.69];p<0.001),相当于相对降低了23.4%。
这些发现突出了全科医生培训师在抗生素处方方面的作用。通过减少抗生素处方并影响下一代全科医生,可以减轻抗生素的人力和经济负担。