Birmingham Women's and Children's Hospital, Birmingham, UK.
King Abdullah International Medical Research Centre, King Saud bin Abdulaziz University for Health Sciences, Genetic Division, Department of Pediatrics, King Abdulaziz Medical City, Ministry of National Guard-Health Affairs (NGHA), Riyadh, Saudi Arabia.
Orphanet J Rare Dis. 2018 Jan 25;13(1):21. doi: 10.1186/s13023-018-0760-3.
In fructose 1,6 bisphosphatase (FBPase) deficiency, management aims to prevent hypoglycaemia and lactic acidosis by avoiding prolonged fasting, particularly during febrile illness. Although the need for an emergency regimen to avoid metabolic decompensation is well established at times of illness, there is uncertainty about the need for other dietary management strategies such as sucrose or fructose restriction. We assessed international differences in the dietary management of FBPase deficiency.
A cross-sectional questionnaire (13 questions) was emailed to all members of the Society for the Study of Inborn Errors of Metabolism (SSIEM) and a wide database of inherited metabolic disorder dietitians.
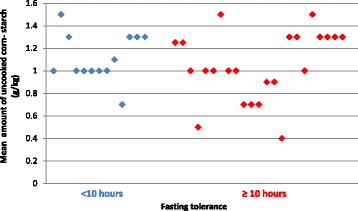
Thirty-six centres reported the dietary prescriptions of 126 patients with FBPase deficiency. Patients' age at questionnaire completion was: 1-10y, 46% (n = 58), 11-16y, 21% (n = 27), and >16y, 33% (n = 41). Diagnostic age was: <1y, 36% (n = 46); 1-10y, 59% (n = 74); 11-16y, 3% (n = 4); and >16y, 2% (n = 2). Seventy-five per cent of centres advocated dietary restrictions. This included restriction of: high sucrose foods only (n = 7 centres, 19%); fruit and sugary foods (n = 4, 11%); fruit, vegetables and sugary foods (n = 13, 36%). Twenty-five per cent of centres (n = 9), advised no dietary restrictions when patients were well. A higher percentage of patients aged >16y rather than ≤16y were prescribed dietary restrictions: patients aged 1-10y, 67% (n = 39/58), 11-16y, 63% (n = 17/27) and >16y, 85% (n = 35/41). Patients classified as having a normal fasting tolerance increased with age from 30% in 1-10y, to 36% in 11-16y, and 58% in >16y, but it was unclear if fasting tolerance was biochemically proven. Twenty centres (56%) routinely prescribed uncooked cornstarch (UCCS) to limit overnight fasting in 47 patients regardless of their actual fasting tolerance (37%). All centres advocated an emergency regimen mainly based on glucose polymer for illness management.
Although all patients were prescribed an emergency regimen for illness, use of sucrose and fructose restricted diets with UCCS supplementation varied widely. Restrictions did not relax with age. International guidelines are necessary to help direct future dietary management of FBPase deficiency.
在果糖-1,6-二磷酸酶(FBPase)缺乏症中,管理的目的是通过避免长时间禁食,尤其是在发热性疾病期间,来预防低血糖和乳酸性酸中毒。尽管在疾病发作时,人们已经清楚地认识到需要制定紧急治疗方案来避免代谢失代偿,但对于其他饮食管理策略(如蔗糖或果糖限制)是否有必要,仍存在不确定性。我们评估了国际上在 FBPase 缺乏症的饮食管理方面的差异。
向所有社会研究先天代谢缺陷协会(SSIEM)成员和广泛的遗传性代谢障碍营养师数据库发送了一份横断面问卷(13 个问题)。
36 个中心报告了 126 例 FBPase 缺乏症患者的饮食处方。完成问卷调查时患者的年龄为:1-10 岁,46%(n=58);11-16 岁,21%(n=27);>16 岁,33%(n=41)。诊断年龄为:<1 岁,36%(n=46);1-10 岁,59%(n=74);11-16 岁,3%(n=4);>16 岁,2%(n=2)。75%的中心主张饮食限制。这包括限制:高蔗糖食物(n=7 个中心,19%);水果和含糖食物(n=4,11%);水果、蔬菜和含糖食物(n=13,36%)。25%的中心(n=9)在患者病情良好时建议不限制饮食。年龄>16 岁的患者中,接受饮食限制的比例高于≤16 岁的患者:1-10 岁,67%(n=39/58);11-16 岁,63%(n=17/27);>16 岁,85%(n=35/41)。随着年龄的增长,具有正常空腹耐受力的患者比例从 1-10 岁的 30%增加到 11-16 岁的 36%,再增加到>16 岁的 58%,但尚不清楚空腹耐受力是否经过生化证实。20 个中心(56%)在 47 例患者中常规使用未经烹饪的玉米淀粉(UCCS)限制夜间禁食,无论其实际空腹耐受力如何(37%)。所有中心都主张采用主要基于葡萄糖聚合物的急症治疗方案来管理疾病。
尽管所有患者都被开了急症治疗方案,但在使用蔗糖和果糖限制饮食加用 UCCS 方面存在很大差异。限制并未随着年龄的增长而放宽。需要制定国际指南,以帮助指导未来 FBPase 缺乏症的饮食管理。