Division of Nephrology and Hypertension, Vanderbilt University Medical Center, Nashville, TN.
Vanderbilt Center for Kidney Disease (VCKD) and Integrated Program for AKI Research (VIP-AKI), Vanderbilt University Medical Center, Nashville, TN.
Crit Care Med. 2018 May;46(5):e380-e388. doi: 10.1097/CCM.0000000000003003.
Acute kidney injury frequently complicates critical illness and is associated with high morbidity and mortality. Frailty is common in critical illness survivors, but little is known about the impact of acute kidney injury. We examined the association of acute kidney injury and frailty within a year of hospital discharge in survivors of critical illness.
Secondary analysis of a prospective cohort study.
Medical/surgical ICU of a U.S. tertiary care medical center.
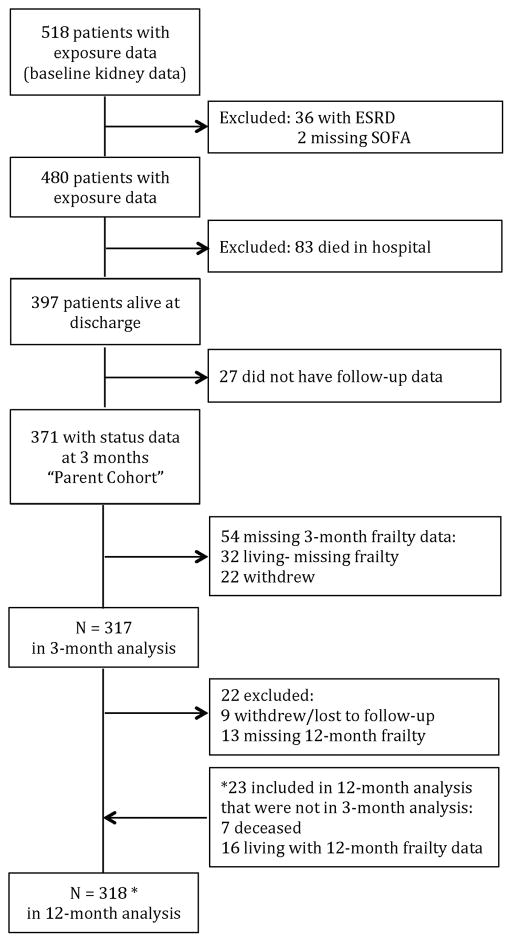
Three hundred seventeen participants with respiratory failure and/or shock.
None.
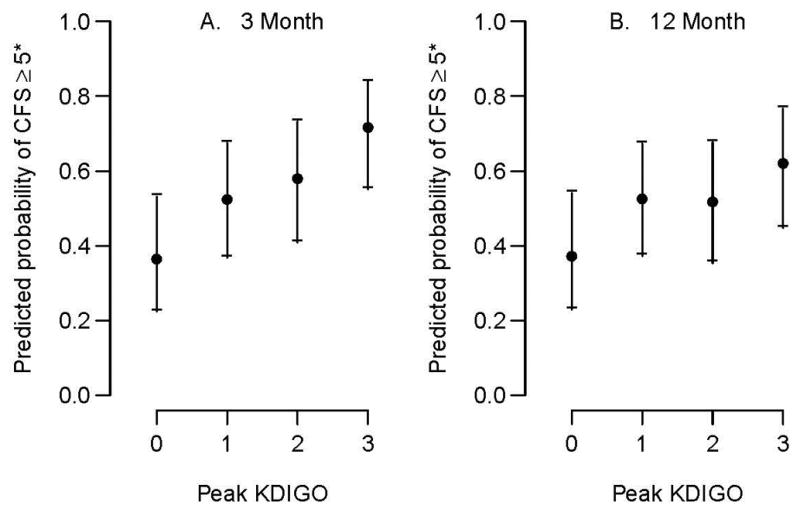
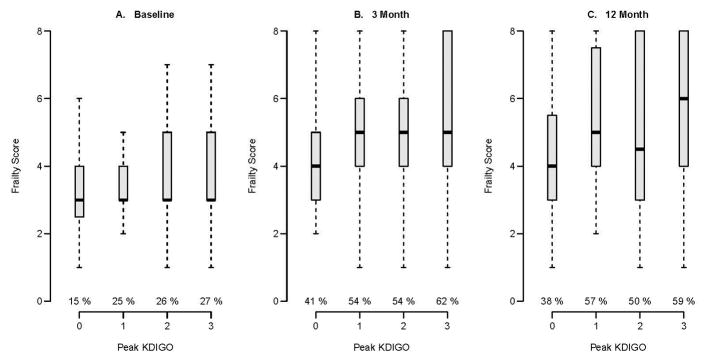
Acute kidney injury was determined using Kidney Disease Improving Global Outcomes stages. Clinical frailty status was determined using the Clinical Frailty Scale at 3 and 12 months following discharge. Covariates included mean ICU Sequential Organ Failure Assessment score and Acute Physiology and Chronic Health Evaluation II score as well as baseline comorbidity (i.e., Charlson Comorbidity Index), kidney function, and Clinical Frailty Scale score. Of 317 patients, 243 (77%) had acute kidney injury and one in four patients with acute kidney injury was frail at baseline. In adjusted models, acute kidney injury stages 1, 2, and 3 were associated with higher frailty scores at 3 months (odds ratio, 1.92; 95% CI, 1.14-3.24; odds ratio, 2.40; 95% CI, 1.31-4.42; and odds ratio, 4.41; 95% CI, 2.20-8.82, respectively). At 12 months, a similar association of acute kidney injury stages 1, 2, and 3 and higher Clinical Frailty Scale score was noted (odds ratio, 1.87; 95% CI, 1.11-3.14; odds ratio, 1.81; 95% CI, 0.94-3.48; and odds ratio, 2.76; 95% CI, 1.34-5.66, respectively). In supplemental and sensitivity analyses, analogous patterns of association were observed.
Acute kidney injury in survivors of critical illness predicted worse frailty status 3 and 12 months postdischarge. These findings have important implications on clinical decision making among acute kidney injury survivors and underscore the need to understand the drivers of frailty to improve patient-centered outcomes.
急性肾损伤常并发于危重病,与高发病率和高死亡率相关。虚弱是危重病幸存者的常见问题,但对于急性肾损伤的影响知之甚少。我们研究了危重病幸存者出院后一年内急性肾损伤和虚弱之间的关系。
前瞻性队列研究的二次分析。
美国一家三级医疗中心的内科/外科重症监护病房。
317 名患有呼吸衰竭和/或休克的患者。
无。
使用肾脏病预后质量倡议(KDIGO)分期确定急性肾损伤。出院后 3 个月和 12 个月时使用临床虚弱量表确定临床虚弱状态。协变量包括平均重症监护器官衰竭评估(SOFA)评分和急性生理学和慢性健康评估 II(APACHE II)评分,以及基线合并症(即 Charlson 合并症指数)、肾功能和临床虚弱量表评分。在 317 名患者中,243 名(77%)患有急性肾损伤,四分之一的急性肾损伤患者在基线时就虚弱。在调整后的模型中,急性肾损伤 1 期、2 期和 3 期与 3 个月时更高的虚弱评分相关(比值比,1.92;95%置信区间,1.14-3.24;比值比,2.40;95%置信区间,1.31-4.42;比值比,4.41;95%置信区间,2.20-8.82)。12 个月时,也观察到急性肾损伤 1 期、2 期和 3 期与更高的临床虚弱量表评分之间存在类似的关联(比值比,1.87;95%置信区间,1.11-3.14;比值比,1.81;95%置信区间,0.94-3.48;比值比,2.76;95%置信区间,1.34-5.66)。在补充和敏感性分析中,观察到类似的关联模式。
危重病幸存者的急性肾损伤预测出院后 3 个月和 12 个月时的虚弱状态更差。这些发现对急性肾损伤幸存者的临床决策具有重要意义,并强调需要了解虚弱的驱动因素,以改善以患者为中心的结局。