Bischoff Sebastian, Walter Thomas, Gerigk Marlis, Ebert Matthias, Vogelmann Roger
Second Department of Internal Medicine, University Medical Center Mannheim, Medical Faculty Mannheim, Heidelberg University, Theodor-Kutzer Ufer 1-3, D-68167, Mannheim, Germany.
Emergency Department, University Medical Center Mannheim, Medical Faculty Mannheim, Heidelberg University, Theodor-Kutzer Ufer 1-3, D-68167, Mannheim, Germany.
BMC Infect Dis. 2018 Jan 26;18(1):56. doi: 10.1186/s12879-018-2960-9.
The aim of this study was to identify clinical risk factors for antimicrobial resistances and multidrug resistance (MDR) in urinary tract infections (UTI) in an emergency department in order to improve empirical therapy.
UTI cases from an emergency department (ED) during January 2013 and June 2015 were analyzed. Differences between patients with and without resistances towards Ciprofloxacin, Piperacillin with Tazobactam (Pip/taz), Gentamicin, Cefuroxime, Cefpodoxime and Ceftazidime were analyzed with Fisher's exact tests. Results were used to identify risk factors with logistic regression modelling. Susceptibility rates were analyzed in relation to risk factors.
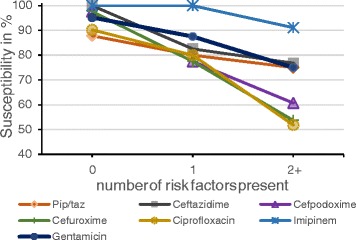
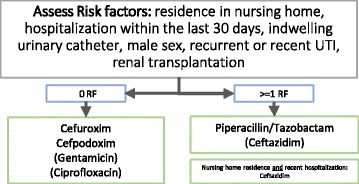
One hundred thirty-seven of four hundred sixty-nine patients who met the criteria of UTI had a positive urine culture. An MDR pathogen was found in 36.5% of these. Overall susceptibility was less than 85% for standard antimicrobial agents. Logistic regression identified residence in nursing homes, male gender, hospitalization within the last 30 days, renal transplantation, antibiotic treatment within the last 30 days, indwelling urinary catheter and recurrent UTI as risk factors for MDR or any of these resistances. For patients with no risk factors Ciprofloxacin had 90%, Pip/taz 88%, Gentamicin 95%, Cefuroxime 98%, Cefpodoxime 98% and Ceftazidime 100% susceptibility. For patients with 1 risk factor Ciprofloxacin had 80%, Pip/taz 80%, Gentamicin 88%, Cefuroxime 78%, Cefpodoxime 78% and Ceftazidime 83% susceptibility. For 2 or more risk factors Ciprofloxacin drops its susceptibility to 52%, Cefuroxime to 54% and Cefpodoxime to 61%. Pip/taz, Gentamicin and Ceftazidime remain at 75% and 77%, respectively.
We identified several risk factors for resistances and MDR in UTI. Susceptibility towards antimicrobials depends on these risk factors. With no risk factor cephalosporins seem to be the best choice for empiric therapy, but in patients with risk factors the beta-lactam penicillin Piperacillin with Tazobactam is an equal or better choice compared to fluoroquinolones, cephalosporins or gentamicin. This study highlights the importance of monitoring local resistance rates and its risk factors in order to improve empiric therapy in a local environment.
本研究旨在确定急诊科尿路感染(UTI)中抗菌药物耐药性和多重耐药(MDR)的临床危险因素,以改善经验性治疗。
对2013年1月至2015年6月急诊科的UTI病例进行分析。采用Fisher精确检验分析对环丙沙星、哌拉西林/他唑巴坦(Pip/taz)、庆大霉素、头孢呋辛、头孢泊肟酯和头孢他啶有或无耐药性的患者之间的差异。结果用于通过逻辑回归模型确定危险因素。分析了药敏率与危险因素的关系。
469例符合UTI标准的患者中,137例尿培养呈阳性。其中36.5%发现有MDR病原体。标准抗菌药物的总体药敏率低于85%。逻辑回归确定养老院居住、男性、过去30天内住院、肾移植、过去30天内抗生素治疗情况、留置导尿管和复发性UTI为MDR或任何这些耐药性的危险因素。对于无危险因素的患者,环丙沙星的药敏率为90%,Pip/taz为88%,庆大霉素为95%,头孢呋辛为98%,头孢泊肟酯为98%,头孢他啶为100%。对于有1个危险因素的患者,环丙沙星的药敏率为80%,Pip/taz为80%,庆大霉素为88%,头孢呋辛为78%,头孢泊肟酯为78%,头孢他啶为83%。对于有2个或更多危险因素的患者,环丙沙星的药敏率降至52%,头孢呋辛降至54%,头孢泊肟酯降至61%。Pip/taz、庆大霉素和头孢他啶分别保持在75%和77%。
我们确定了UTI中耐药性和MDR的几个危险因素。对抗菌药物的药敏性取决于这些危险因素。无危险因素时,头孢菌素似乎是经验性治疗的最佳选择,但对于有危险因素的患者,β-内酰胺类青霉素哌拉西林/他唑巴坦与氟喹诺酮类、头孢菌素类或庆大霉素相比是同等或更好的选择。本研究强调了监测当地耐药率及其危险因素以改善当地环境中经验性治疗的重要性。