Medical ICU, Peking Union Medical College Hospital, Peking Union Medical College and Chinese Academy of Medical Sciences, 1 Shuai Fu Yuan, Beijing, 100730, People's Republic of China.
Department of Critical Care Medicine, the First Affiliated Hospital of Fujian Medical University, 20 Chazhong Road, Fuzhou, 350000, People's Republic of China.
Crit Care. 2018 Jan 28;22(1):20. doi: 10.1186/s13054-017-1937-1.
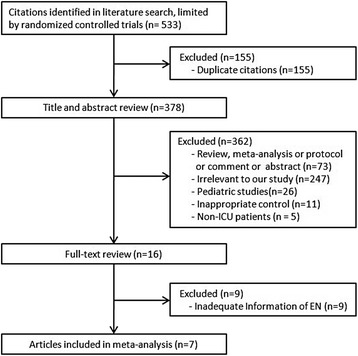
Pharmacologic stress ulcer prophylaxis (SUP) is recommended in critically ill patients with high risk of stress-related gastrointestinal (GI) bleeding. However, as to patients receiving enteral feeding, the preventive effect of SUP is not well-known. Therefore, we performed a meta-analysis of randomized controlled trials (RCTs) to evaluate the effect of pharmacologic SUP in enterally fed patients on stress-related GI bleeding and other clinical outcomes.
We searched PubMed, Embase, and the Cochrane database from inception through 30 Sep 2017. Eligible trials were RCTs comparing pharmacologic SUP to either placebo or no prophylaxis in enterally fed patients in the ICU. Results were expressed as risk ratio (RR) and mean difference (MD) with accompanying 95% confidence interval (CI). Heterogeneity, subgroup analysis, sensitivity analysis and publication bias were explored.
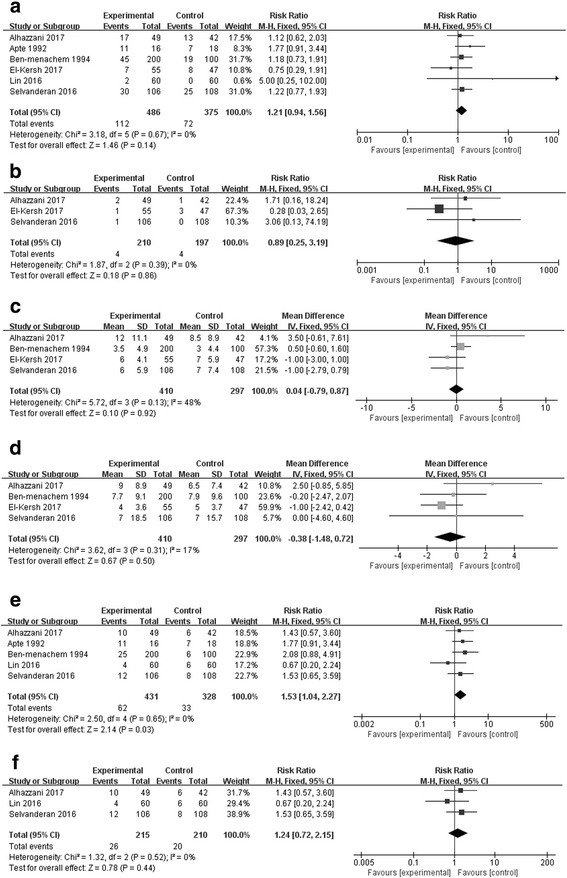
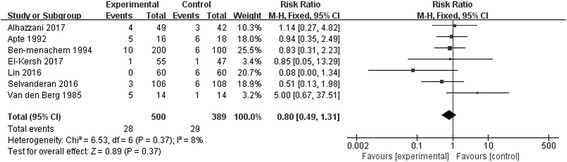
Seven studies (n = 889 patients) were included. There was no statistically significant difference in GI bleeding (RR 0.80; 95% CI, 0.49 to 1.31, p = 0.37) between groups. This finding was confirmed by further subgroup analyses and sensitivity analysis. In addition, SUP had no effect on overall mortality (RR 1.21; 95% CI, 0.94 to 1.56, p = 0.14), Clostridium difficile infection (RR 0.89; 95% CI, 0.25 to 3.19, p = 0.86), length of stay in the ICU (MD 0.04 days; 95% CI, -0.79 to 0.87, p = 0.92), duration of mechanical ventilation (MD -0.38 days; 95% CI, -1.48 to 0.72, p = 0.50), but was associated with an increased risk of hospital-acquired pneumonia (RR 1.53; 95% CI, 1.04 to 2.27; p = 0.03).
Our results suggested that in patients receiving enteral feeding, pharmacologic SUP is not beneficial and combined interventions may even increase the risk of nosocomial pneumonia.
对于有发生应激性胃肠道(GI)出血高危风险的重症患者,推荐使用药物性应激性溃疡预防(SUP)。然而,对于接受肠内喂养的患者,SUP 的预防效果尚不清楚。因此,我们对随机对照试验(RCT)进行了荟萃分析,以评估药物性 SUP 在接受肠内喂养的 ICU 患者中对应激性 GI 出血和其他临床结局的影响。
我们从建库至 2017 年 9 月 30 日检索了 PubMed、Embase 和 Cochrane 数据库。纳入的试验为比较药物性 SUP 与安慰剂或无预防措施在 ICU 中接受肠内喂养的患者之间的 RCT。结果以风险比(RR)和均值差(MD)及相应的 95%置信区间(CI)表示。探索了异质性、亚组分析、敏感性分析和发表偏倚。
纳入了 7 项研究(n=889 例患者)。两组间 GI 出血无统计学差异(RR 0.80;95% CI,0.49 至 1.31,p=0.37)。这一发现通过进一步的亚组分析和敏感性分析得到了证实。此外,SUP 对总体死亡率(RR 1.21;95% CI,0.94 至 1.56,p=0.14)、艰难梭菌感染(RR 0.89;95% CI,0.25 至 3.19,p=0.86)、ICU 住院时间(MD 0.04 天;95% CI,-0.79 至 0.87,p=0.92)、机械通气时间(MD -0.38 天;95% CI,-1.48 至 0.72,p=0.50)无影响,但与医院获得性肺炎的风险增加相关(RR 1.53;95% CI,1.04 至 2.27;p=0.03)。
我们的结果表明,对于接受肠内喂养的患者,药物性 SUP 并无益处,联合干预甚至可能增加医院获得性肺炎的风险。