Gesesew Hailay Abrha, Ward Paul, Woldemichael Kifle, Mwanri Lillian
Public Health, Flinders University, Adelaide, Australia.
Epidemiology, Jimma University, Jimma, Ethiopia.
BMC Infect Dis. 2018 Jan 30;18(1):59. doi: 10.1186/s12879-018-2971-6.
Early presentation for HIV care is vital as an initial tread in the UNAIDS 90-90-90 targets. However, late presentation for HIV care (LP) challenges achieving the targets. This study assessed the prevalence, trends, outcomes and risk factorsfor LP.
A 12 year retrospective cohort study was conducted using electronic medical records extracted from an antiretroviral therapy (ART) clinic at Jimma University Teaching Hospital. LP for children refers to moderate or severe immune-suppression, or WHO clinical stage 3 or 4 at the time of first presentation to the ART clinics. LP for adults refers to CD4 lymphocyte count of < 200 cells/ μl and < 350 cells/μl irrespective of clinical staging, or WHO clinical stage 3 or 4 irrespective of CD4 count at the time of first presentation to the ART clinics. Binary logistic regression was used to identify factors that were associated with LP, and missing data were handled using multiple imputations.
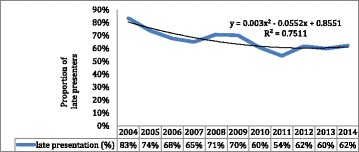
Three hundred ninety-nine children and 4900 adults were enrolled in ART care between 2003 and 15. The prevalence of LP was 57% in children and 66.7% in adults with an overall prevalence of 65.5%, and the 10-year analysis of LP showed upward trends. 57% of dead children, 32% of discontinued children, and 97% of children with immunological failure were late presenters for HIV care. Similarly, 65% of dead adults, 65% of discontinued adults, and 79% of adults with immunological failure presented late for the care. Age between 25- < 50 years (AOR = 0.4,95% CI:0.3-0.6) and 50+ years (AOR = 0.4,95% CI:0.2-0.6), being female (AOR = 1.2, 95% CI: 1.03-1.5), having Tb/HIV co-infection (AOR = 1.6, 95% CI: 1.09-2.1), having no previous history of HIV testing (AOR = 1.2, 95% CI: 1.1-1.4), and HIV care enrollment period in 2012 and after (AOR = 0.8, 95% CI: 0.7-0.9) were the factors associated with LP for Adults. For children, none of the factors were associated with LP.
The prevalence of LP was high in both adults and children. The majority of both children and adults who presented late for HIV care had died and developed immunological failure. Effective programs should be designed and implemented to tackle the gap in timely HIV care engagement.
尽早接受艾滋病护理对于实现联合国艾滋病规划署90-90-90目标至关重要。然而,晚期接受艾滋病护理(LP)对实现这些目标构成挑战。本研究评估了LP的患病率、趋势、结局及危险因素。
利用从吉姆马大学教学医院抗逆转录病毒治疗(ART)诊所提取的电子病历进行了一项为期12年的回顾性队列研究。儿童的LP是指首次到ART诊所就诊时出现中度或重度免疫抑制,或世界卫生组织临床分期为3期或4期。成人的LP是指首次到ART诊所就诊时,无论临床分期,CD4淋巴细胞计数<200个细胞/μl和<350个细胞/μl,或无论CD4计数,世界卫生组织临床分期为3期或4期。采用二元逻辑回归确定与LP相关的因素,并使用多重插补法处理缺失数据。
2003年至2015年期间,399名儿童和4900名成人接受了ART治疗。儿童LP的患病率为57%,成人LP的患病率为66.7%,总体患病率为65.5%,对LP的10年分析显示呈上升趋势。57%的死亡儿童、32%的中断治疗儿童以及97%的免疫功能衰竭儿童为晚期接受艾滋病护理者。同样,65%的死亡成人、65%的中断治疗成人以及79%的免疫功能衰竭成人就诊较晚。25-<50岁(调整后比值比[AOR]=0.4,95%置信区间[CI]:0.3-0.6)和50岁及以上(AOR=0.4,95%CI:0.2-0.6)、女性(AOR=1.2,95%CI:1.03-1.5)、合并结核/艾滋病感染(AOR=1.6,95%CI:1.09-2.1)、既往无艾滋病检测史(AOR=1.2,95%CI:1.1-1.4)以及2012年及以后的艾滋病护理入组时间(AOR=0.8,95%CI:0.7-0.9)是与成人LP相关的因素。对于儿童,没有因素与LP相关。
成人和儿童中LP的患病率均较高。大多数晚期接受艾滋病护理的儿童和成人已经死亡并出现了免疫功能衰竭。应设计并实施有效的项目来解决及时接受艾滋病护理方面的差距。