Division of Pulmonary, Critical Care, and Sleep Medicine, Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, NY.
Department of Emergency Medicine, Icahn School of Medicine at Mount Sinai, New York, NY.
Crit Care Med. 2018 May;46(5):720-727. doi: 10.1097/CCM.0000000000002993.
ICU admission delays can negatively affect patient outcomes, but emergency department volume and boarding times may also affect these decisions and associated patient outcomes. We sought to investigate the effect of emergency department and ICU capacity strain on ICU admission decisions and to examine the effect of emergency department boarding time of critically ill patients on in-hospital mortality.
A retrospective cohort study.
Single academic tertiary care hospital.
Adult critically ill emergency department patients for whom a consult for medical ICU admission was requested, over a 21-month period.
None.
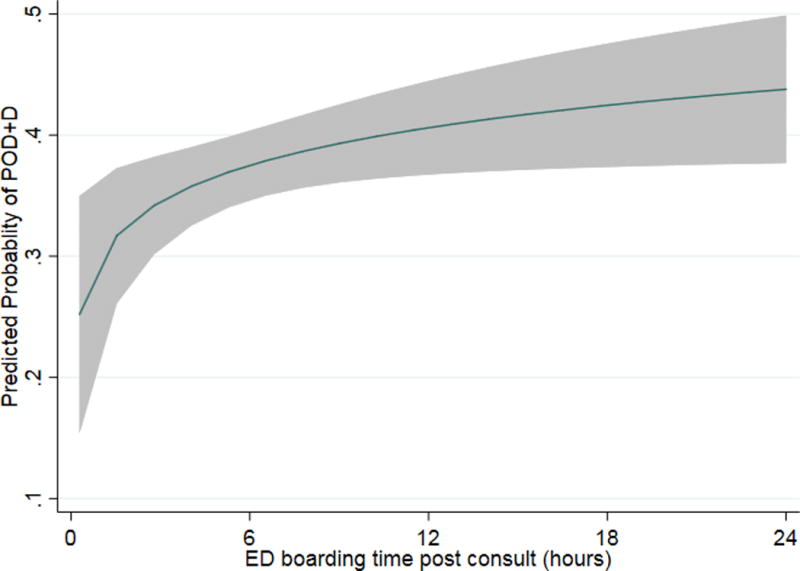
Patient data, including severity of illness (Mortality Probability Model III on Admission), outcomes of mortality and persistent organ dysfunction, and hourly census reports for the emergency department, for all ICUs and all adult wards were compiled. A total of 854 emergency department requests for ICU admission were logged, with 455 (53.3%) as "accept" and 399 (46.7%) as "deny" cases, with median emergency department boarding times 4.2 hours (interquartile range, 2.8-6.3 hr) and 11.7 hours (3.2-20.3 hr) and similar rates of persistent organ dysfunction and/or death 41.5% and 44.6%, respectively. Those accepted were younger (mean ± SD, 61 ± 17 vs 65 ± 18 yr) and more severely ill (median Mortality Probability Model III on Admission score, 15.3% [7.0-29.5%] vs 13.4% [6.3-25.2%]) than those denied admission. In the multivariable model, a full medical ICU was the only hospital-level factor significantly associated with a lower probability of ICU acceptance (odds ratio, 0.55 [95% CI, 0.37-0.81]). Using propensity score analysis to account for imbalances in baseline characteristics between those accepted or denied for ICU admission, longer emergency department boarding time after consult was associated with higher odds of mortality and persistent organ dysfunction (odds ratio, 1.77 [1.07-2.95]/log10 hour increase).
ICU admission decisions for critically ill emergency department patients are affected by medical ICU bed availability, though higher emergency department volume and other ICU occupancy did not play a role. Prolonged emergency department boarding times were associated with worse patient outcomes, suggesting a need for improved throughput and targeted care for patients awaiting ICU admission.
入住 ICU 时间延迟可能会对患者预后产生负面影响,但急诊科的工作量和住院时间也可能会影响这些决策和相关患者的预后。我们旨在研究急诊科和 ICU 容量负荷对 ICU 收治决策的影响,并探讨危重症患者急诊科住院时间对院内死亡率的影响。
回顾性队列研究。
单家学术性三级护理医院。
在 21 个月期间,因 ICU 收治咨询而入住急诊科的成年危重症患者。
无。
收集了患者数据,包括入院时的严重程度(III 型死亡率预测模型)、死亡率和持续器官功能障碍的结果,以及急诊科、所有 ICU 和所有成人病房的每小时人员统计报告。共记录了 854 例 ICU 收治咨询请求,其中 455 例(53.3%)为“接受”,399 例(46.7%)为“拒绝”,急诊留观时间中位数分别为 4.2 小时(四分位间距,2.8-6.3 小时)和 11.7 小时(3.2-20.3 小时),持续器官功能障碍和/或死亡率分别为 41.5%和 44.6%。接受治疗的患者年龄较小(平均±标准差,61±17 岁比 65±18 岁)且病情更严重(入院时 III 型死亡率预测模型评分中位数,15.3%[7.0-29.5%]比 13.4%[6.3-25.2%])。在多变量模型中,只有满员的 ICU 是与 ICU 收治可能性降低显著相关的唯一医院层面因素(比值比,0.55[95%CI,0.37-0.81])。通过使用倾向评分分析来平衡 ICU 收治接受或拒绝患者之间的基线特征差异,咨询后急诊留观时间延长与死亡率和持续器官功能障碍的可能性增加相关(比值比,1.77[1.07-2.95]/log10 小时增加)。
危重症急诊科患者的 ICU 收治决策受 ICU 床位可用性的影响,尽管急诊科工作量增加和其他 ICU 占用率并未发挥作用。延长急诊科留观时间与患者预后恶化相关,提示需要改善 ICU 收治等待患者的流程并对其进行有针对性的治疗。